Discover how TripLog can drive time and cost savings for your company.
TripLog is the market’s premier mileage and expense tracking solution. We cater to businesses of all sizes and industries. Find out how much your company can save:
Learn about new features, tips & tricks, and how people have used TripLog to save thousands of dollars and man-hours.
- What’s new

EVV Compliance Requirements by State (2024 Update)

Dimitri Gedevanishvili

The 21st Century Cures Act included a federal mandate requiring healthcare providers to use electronic visit verification, or EVV. Individual states continue to roll out their solutions as only a small number managed to meet the January 1, 2020 deadline.
As of January 1, 2023, all agencies must have implemented EVV, including home healthcare companies. Home healthcare may not be covered by Medicaid if the agency has not implemented an EVV solution.
Each state is able to choose how it wants to collect and disclose EVV data. They may also choose how detailed they want their state-level compliance regulations to be.
Related: Mileage Reimbursement For Healthcare Companies
EVV Methods Explained
States have a few methods of EVV to choose from:
- Open vendor: States are able to select an EVV vendor and a data aggregator. Organizations and providers are able to use these state-sponsored vendors free of charge, though they can also work with a different EVV vendor at their own expense. Generally speaking, if your org utilizes an alternative vendor, it will need to integrate with the state’s choice of data aggregator.
- State-mandated external vendor: Providers are required to use a specific state-sponsored and funded vendor.
- State-mandated in-house system: States may contract and build their own EVV systems that providers must use.
- Provider choice: Providers must choose their own vendors and cover the costs themselves. Since this puts all of the cost on the organizations, some states may raise reimbursement rates to help offset these costs.
- Managed care organization (MCO) choice: MCOs will select the vendor and cover the costs. They may or may not receive state support to assist with the costs.
The majority of states are selecting state-sponsored vendors. EVV systems operated by the state or a state-sponsored vendor may qualify for additional federal financial assistance.
There are a few methods for EVV verification, including:
- Dedicated EVV devices in their client’s homes
- GPS-enabled mobile apps that the caregivers use
- Toll-free numbers that providers call from the client’s home phone
Why is EVV required now – and what could it mean for the future?
The reason the federal government has chosen to mandate EVV is to reduce fraud and save providers (as well as their patients) money. EVV systems track the type of service performed, which individual is receiving care, and the provider, as well as the date, location, and time of the service.
Many states are choosing different ways to deploy EVV, usually regarding fears and skepticism of the new regulation, worries over privacy violations, and concerns over the privacy and security of their providers.
Related: Home Health Care Mileage Reimbursement – Why Companies Should Care
Some may view EVV as government overreach. Others feel as though the intricate tracking of providers may result in unsafe working conditions. Regardless, the requirements to implement EVV are here, and it is up to you to get your organization compliant based on your individual state’s regulations.

EVV Requirements By State
Alabama evv requirements.
EVV model: Open vendor
As of February 14, 2022, Alabama uses an open-model modular EVV system with HHAeXchange . This is designed to be a free EVV system for providers of personal and home healthcare services. Agencies may still use a third-party EVV solution, but they will need to import data to the HHAeXchange using Electronic Data Interchange.
Alaska EVV Requirements
Alaska’s state-sponsored EVV vendor and data aggregator is Therap . If an agency wants to use a different EVV vendor, it must be approved by Therap to ensure that it can integrate with Therap’s data aggregation solution. Licensed providers are able to use Therap’s EVV solutions at no cost to them.
Arizona EVV Requirements
Arizona uses Sandata as its state-sponsored EVV vendor and data aggregator. Agencies may use other vendors for EVV at their own expense, but they will need to submit their data to Sandata.
Arkansas EVV Requirements
Arkansas chose AuthentiCare as its EVV model, but providers may use third-party systems as long as they use AuthentiCare as the data aggregator.
California EVV Requirements
California uses CalEVV as its state-provided EVV model. Providers may use a different EVV system if they choose, as long as its data is able to integrate with CalEVV.
Colorado EVV Requirements
EVV has been mandatory in Colorado since August 2020. Agencies may use Colorado’s provided EVV solution, Sandata , at no cost to them, though they may utilize a different system at their own expense. Providers who do this must ensure that their system follows Colorado’s specific EVV regulations.
Connecticut EVV Requirements
EVV model: State-mandated external vendor
Connecticut requires agencies to use Sandata as their vendor.
Delaware EVV Requirements
On February 1, 2022, it was announced that Delaware chose Sandata as its official EVV vendor. Providers may use Sandata free of charge, or they can use their own EVV system as long as it feeds data into Sandata.
Florida EVV Requirements
Florida uses Tellus as its EVV vendor, a subsidiary of Netsmart . However, as Florida uses an open vendor system, agencies may choose to use a different vendor.
Georgia EVV Requirements
Georgia is still in the process of implementing its EVV system for home healthcare services, having missed the January 1, 2023 deadline . Georgia uses Netsmart as its EVV solution.
Hawaii EVV Requirements
Providers in Hawaii may use its state-sponsored vendor Sandata free of charge, or they can choose an alternative EVV vendor as long as it integrates with Sandata’s data aggregator.
Idaho EVV Requirements
EVV model: Provider choice
Idaho follows the provider choice EVV model , though it uses Sandata as its data aggregator. Providers must choose a provider at their own expense that has a verified integration with Sandata .
Illinois EVV Requirements
Illinois uses Santrax as its EVV solution . As this is its state-mandated vendor, agencies do not have a choice to use another EVV solution or data aggregator.
Indiana EVV Requirements
Indiana has chosen Sandata as its method of implementing federal EVV requirements. As with most other open vendor models, providers may use alternative EVV solutions if they integrate with Sandata’s data aggregator.
Iowa EVV Requirements
Iowa uses CareBridge as its EVV method . Providers may use CareBridge free of charge, though they have the option to choose an alternative method as long as it integrates with CareBridge’s data aggregator.
Kansas EVV Requirements
Kansas uses AuthentiCare as its EVV provider. As Kansas uses the state-mandated model, agencies cannot use any other EVV systems.
Kentucky EVV Requirements
Kentucky uses Netsmart as its free state-sponsored EVV provider and data aggregator, though healthcare organizations may use another vendor at their discretion, as long as it is state-approved.
Louisiana EVV Requirements
Louisiana uses an EVV provider called the “Louisiana State Reporting System” (LaSRS) . However, like most other open vendor models, providers may use other EVV vendors as long as their data integrates with LaSRS.
Maine EVV Requirements
Maine uses Sandata as its EVV provider . Providers can use it free of charge or use their own system at their own expense. EVV records will still need to be submitted to Sandata’s data aggregator .
Maryland EVV Requirements
EVV Model: State-mandated in-house system
Maryland has used its state-mandated EVV system for a number of years now. Known as the “ In-Home Supports Assurance System ” (ISAS), providers are required to use this system in the state of Maryland.
Massachusetts EVV Requirements
Massachusetts offers Optum as its EVV vendor . Providers may use it free of charge, though they may use another provider if it is able to integrate with Optum’s data aggregator.
Michigan EVV Requirements
Michigan intends to offer a state-sponsored EVV provider, but as of March 2023, they still have not finalized the details . For now, healthcare providers are able to choose their own EVV solution.
Minnesota EVV Requirements
Minnesota uses HHAeXchange as its EVV vendor . Providers may use other vendors as long as they connect with HHAeXchange’s data aggregator.
Mississippi EVV Requirements
As of February 21st, 2023, Mississippi has moved from a closed model to an open vendor model , offering HHAeXchange as its EVV provider and data aggregator.
Missouri EVV Requirements
Mississippi uses Sandata as its EVV vendor and data aggregator. Healthcare providers may use Sandata free of charge, or use their own solution at their own expense, as long as it integrates with Sandata’s data aggregator.
Montana EVV Requirements
Montana has chosen Netsmart as its free EVV vendor , though through the open vendor model, providers may choose a different vendor if they so choose. The vendor will need to integrate with Netsmart’s data aggregator, however.
This system is not yet in place at the time of this writing, with Montana’s DPHHS expecting the system to be implemented in September 2023.
Nebraska EVV Requirements
Nebraska uses Netsmart as its free EVV provider . You may use a third-party solution as long as it integrates with Netsmart’s data aggregator.
Nevada EVV Requirements
Nevada requires healthcare providers to use AuthentiCare as their EVV provider.
New Hampshire EVV Requirements
As of March 2023, New Hampshire is currently in the process of setting up its free EVV solution. They have contracted First Data Government Solutions LP as their EVV provider, though healthcare orgs can pick their own EVV solution, as long as it syncs with First Data’s data aggregator.
New Jersey EVV Requirements
New Jersey uses HHAeXchange as its EVV vendor . With that said, providers may choose their own EVV solution as long as it syncs with HHAeXchange’s data aggregator.
New Mexico EVV Requirements
New Mexico requires healthcare orgs to use AuthentiCare as its EVV provider.
New York EVV Requirements
With the provider choice model in place, the state of New York does not offer a free EVV solution . Providers will need to investigate and choose an EVV solution at their own discretion and expense. The state does provide a data aggregator, however, and providers will need to sync their EVV solution’s data to it.
North Carolina EVV Requirements
North Carolina provides Sandata as its free EVV solution . Through the open vendor model, providers may choose their own solution as long as it syncs with Sandata’s data aggregator.
North Dakota EVV Requirements
North Dakota uses Therap as its EVV solution , letting healthcare orgs use it free of charge. However, providers may use their own EVV system as long as their data can be submitted to the proper data aggregator.
Ohio EVV Requirements
Ohio offers Sandata as its free-of-charge state-provided EVV vendor , though alternatives may be used as long as it integrates with Sandata’s data aggregator.
Oklahoma EVV Requirements
Oklahoma offers AuthentiCare as its EVV provider . Oklahoma used to use a state-mandated system, but it appears as though it is moving to an open vendor system in which other EVV solutions may be used, as long as they feed into AuthentiCare’s data aggregator.
Oregon EVV Requirements
EVV model: State-mandated in-house system
Oregon built an EVV system into its Express Payment and Reporting System (eXPRS) . Healthcare providers are still allowed to choose alternative solutions as long as their data uploads to eXPRS.
Pennsylvania EVV Requirements
Pennsylvania is working with Sandata to provide an EVV solution free of charge to providers in the state. With that said, providers may choose alternative solutions as long as they integrate with Sandata’s data aggregator.
Rhode Island EVV Requirements
Rhode Island uses Sandata as its state-provided EVV vendor and data aggregator. However, providers may use other vendors that integrate with Sandata’s data aggregator.
South Carolina EVV Requirements
South Carolina requires providers to use AuthentiCare for EVV. However, it appears that the state’s EVV implementation has been postponed .
South Dakota EVV Requirements
South Dakota offers Therap as its EVV provider . However, other providers are working with the state to potentially offer EVV solutions as well.
Tennessee EVV Requirements
Tennessee appears to offer Sandata as its EVV provider , but other solutions are working with the state to offer EVV as well.
Texas EVV Requirements
EVV model: State-mandated external vendors
Unlike most states, Texas offers a pool of a few EVV vendors that providers can choose from.
Utah EVV Requirements
Utah does not offer a free EVV provider , requiring healthcare orgs to choose a vendor at their own discretion and expense.
Vermont EVV Requirements
Vermont uses Sandata as its free EVV provider and data aggregator . With that said, Vermont healthcare companies may choose other providers as long as they sync with Sandata’s data aggregator.
Virginia EVV Requirements
Virginia is a “provider choice” state , meaning that providers may choose the EVV system that they feel will work best for them.
Washington state EVV Requirements
Washington state uses the “provider choice” model , which requires healthcare providers to choose their own EVV systems. They will need to connect to ProviderOne, which is Washington state’s data aggregator.
Washington, D.C. EVV Requirements
Washington, D.C. provides Sandata as its free EVV solution , though third-party vendors may be used that sync with Sandata’s data aggregator.
West Virginia EVV Requirements
West Virginia offers HHAeXchange as its free EVV solution , though providers may use other solutions as long as they integrate with HHAeXchange’s data aggregator.
Wisconsin EVV Requirements
Wisconsin uses Sandata as its free EVV solution . Agencies can use other third-party solutions as long as they integrate with Sandata’s data aggregator.
Wyoming EVV Requirements
Wyoming offers CareBridge as its free EVV solution , but healthcare providers may choose other EVV solutions as long as they sync with CareBridge’s data aggregator.
We hope this guide has helped you better understand your state’s specific EVV requirements. For a solution that folds EVV, mileage, expense, and time tracking all in one, look no further than TripLog!
Schedule a complimentary live demo to see if TripLog is the right solution for your organization.
Like what you read?
Show that you found the article interesting by liking and sharing.

Ditch manual mileage and expense reports and save thousands with TripLog!

Fixed and Variable Rate (FAVR) Reimbursement Programs Explained | How To Implement a FAVR Program

Free Uber/Lyft Vehicle Inspections Explained (2024 update)

Best Times to Deliver For Uber Eats (2024 Guide)
Switch to the #1 mileage tracking & reimbursement solution.

(4.8 rating score)
Mileage Tracking For Companies
Mileage Tracking For Self-Employed
Feature Videos
TripLog Drive™
TripLog Beacon ™
ACH Reimbursement
Company Debit Cards
Bank/Credit Cards
Google & Outlook Calendar
Emburse (Certify & Chrome River)
Sage Intacct
Construction
Public Sector & Nonprofits
Sales Representatives
Accountants
Login with Intuit
Terms of Service
Privacy Policy
© 2011 – 2024 Copyright TripLog, Inc. All Rights Reserved.
Let's chat!
Number of anticipated TripLog users:
Need support?
Mileage Reimbursement Savings Calculator
Using outdated manual mileage logs can cost businesses thousands of dollars per year in lost time and incorrect reimbursements . See how much TripLog can help you save!
Number of drivers
Average miles daily per person
Number of trips daily
Cents-per-mile
Annual mileage reimbursement costs based on the numbers you provided.
Annual Mileage Reimbursement
50 mi/day x 100 drivers x $0.54 (5 days x 50 wks)
This is the inline help tip! You can explain to your users what this section of your web app is about.
According to research, on average employees inflate the mileage by 25% when self reported.
Estimated Reimbursement Savings
People on average spend 2 minutes on manually recording trips.
Manual Entry Hours
2 mins x 10 trips/day x 100 drivers (5 days x 50 wks)
Taking national average $25 hourly rate.
Estimated Labor Savings
Avg. $25/hr x Manual Entry Hours
Your Company
(Labor Savings + Reimbursement Savings) / Number of Drivers
Before you go, schedule a complimentary demo
See how TripLog works, ask questions, and explore your potential savings!
Get TripLog
Start automatically tracking your mileage today to never miss another deductible mile. Try the #1 mileage tracker for free!
(4.8 out of 5)
Schedule a call with a TripLog agent in as little as 15 minutes!
In your introductory meeting with one of our mileage experts, you will:
- Get a demo of the TripLog admin dashboard.
- Have the opportunity to ask questions.
- Learn more about how TripLog can benefit your team.
- Get insight into which pricing plan will best suit your team’s needs.
- Sponsor-Ad Rates
- Career Center
- Adult Day Health Care
- Assisted Living and Adult Care Facilities
- Continuing Care Retirement Communities
- Home and Community-Based Services
- Managed Long Term Care
- Nursing Homes
- Retirement Housing
- Biweekly Member Calls
- Coronavirus Resources
- Infectious Disease Resources
- Workforce Issues and Regulations
- State Councils and Task Forces
- Diversity, Equity, and Inclusion
- Value-Based Payment
- Medicaid Redesign
- Grants and Research
- Events & Education
- LeadingAge Quality Metrics
- LeadingAge New York FASTracker
- Value First Group Purchasing
- Young at Heart
- Energy Consulting
- Endorsed Vendor Program
- LeadingAge New York Business Partners
- LeadingAge New York Consumer Guide
- Sponsorship and Advertising Rates
- Intelligence
- Legislative Bulletin
- Solutions Newsletter
- Sponsorships & Partner Packages
- 2023 Membership Directory
- 2024 Consumer Guide
- » Providers
- » Home and Community-Based Services
- » Electronic Visit Verification
- » CMS Issues New FAQ on Electronic Visit Verification
CMS Issues New FAQ on Electronic Visit Verification
The Centers for Medicare and Medicaid Services (CMS) has released new guidance, including a new Frequently Asked Questions document, on the mandate that states require electronic visit verification (EVV) for personal care services by January 1, 2020 and for home health care services by January 1, 2023. The guidance is at https://www.medicaid.gov/federal-policy-guidance/downloads/cib080819-2.pdf .
The FAQ addresses EVV applicability regarding beneficiaries with live-in caregivers, services delivered partially in the beneficiary’s home, and the provision of medical supplies, equipment, and appliances as a component of the Medicaid home health benefit. It clarifies that web-based electronic timesheets with dual verification are not a permissible form of EVV as they do not provide the state with auditable confirmation of the data entered by the provider and approved by the individual.
The FAQ also clarifies that EVV is only required for the portion of the service rendered in the home; however, states may choose to require more information to control fraud, waste, and abuse. It offers various methods of verification as options for alleviating privacy concerns regarding tracking of community locations while ensuring that the location of any portion of a service delivered in the home is recorded. States may select the approach that best aligns with their systems and program integrity goals.
The Department of Health intends to make a request to CMS that EVV implementation for personal care services be delayed for one year, from January 1, 2020 to January 1, 2021. The EVV statute allows states to seek up to one year of additional implementation time if they can demonstrate they have made a good-faith effort to comply and have encountered unavoidable delays.
To obtain more information on the EVV requirement, click here. For questions or concerns, email [email protected] . LeadingAge New York will keep members updated as New York proceeds with its own implementation plan for EVV.
Contact: Meg Everett, [email protected] , 518 867-8871.
13 British American Blvd Suite 2 Latham, NY 12110 518.867.8383 518.867.8384 fax
- LeadingAge New York
- LeadingAge NY Services Inc.
- Foundation for Long Term Care
- Adult Day Health Care Council
- Terms & Conditions
- Report Abuse
- Report Fraud
- eDocs document library
Contact DHS
- eDocs and forms
- Items on PartnerLink
- Paper document bulk ordering
Make online payments
Report abuse
Report fraud
Respond to an RFP
EVV provider FAQ
Below are answers to frequently asked questions about electronic visit verification for providers. You may also download an accessible PDF version of this FAQ .
December EVV quarterly session
Responses to questions raised at the Dec. 11, 2023, session:
DHS has previously announced that the soft launch for all phases of EVV will continue into 2024. At this time, DHS expects that provider agencies are onboarding their members and caregivers to the EVV system and are sending EVV visit data through their EVV system.
You can find more information on getting started by going to the DHS EVV website and following the directions under the "Providers" tab. Look for “First step for all providers” to find common answers and directions for next steps, including links to the HHAeXchange enrollment surveys.
All providers must complete an enrollment survey whether they choose to use the state EVV system or a third-party system.
The email used to complete the survey will be the email used to receive communication from HHAX. If you need to update an email address, contact HHAX.
Services requiring EVV
Both straight MA and MA through an MCO require EVV.
If the service has a specific remote modifier, then EVV would not be required. Otherwise, they will need to select Community.
Review the DHS EVV website under the “Required services” tab. If the service is listed, then EVV is required. If the service is not listed, EVV is not required at this time.
When the caregiver is clocking in and out in the HHAeXchange mobile app, they will have the option to select a community checkbox when they are outside of the 500-foot geofence. Please contact HHAX via their client support portal if you cannot find the community checkbox.
No. The geofence is not a barrier to receiving services and does not prevent the person from receiving services wherever they go. DHS needs to be able to identify when a person is receiving services at “home” vs. when they are receiving services in the “community.”
Service authorizations
Providers may check a member’s eligibility and health plan status in MN-ITS. MN-ITS will note if a member is enrolled with a prepaid health plan.
No, you do not need to wait. You may manually enter the information into HHAX.
Contact the EVV team using the DSD Contact form and include your HHAX ticket numbers.
Members not showing up in portal
If your agency is missing members who are authorized to receive services that require EVV, do the following:
- Provider agencies may have different offices for the different types of services provided. Please confirm that your agency has accurately reported to HHAX all the services that your agency provides along with all UMPI/NPI numbers and any site-specific taxonomy codes. If you need to update this, contact HHAX via the support portal.
- Review the list of EVV required services to confirm that EVV is required. Note the modifiers.
- If the service being provided does not require a prior authorization (many home health services and some services with MCOs) there will not be a member profile or an authorization to flow into the system. In these cases, providers will manually create the member profile and the authorization.
- Confirm your agency has an ACTIVE authorization for the individual(s) you’re missing.
- Confirm the missing individual(s) has ACTIVE MA/health plan.
In most cases, the above steps will identify the issue. If the issue persists, contact HHAX via the support portal.
Contact HHAX and provide them your UMPI number and ask them to create a waiver office for your program.
Consult the training materials in your provider portal and in the HHAeXchange learning management system (LMS).
HHAX questions
When you use the HHAX Client Support Portal , we recommend allowing HHAX some time to address your inquiry. Be patient and allow the support team up to 10 business days to respond.
Reach out to HHAX using the HHAX Client Support Portal .
This recording will be posted on the Electronic Visit Verification (EVV) quarterly updates page. Scroll down the webpage (about halfway) until you see the “Electronic Visit Verification (EVV)” header.
The answers to questions asked at quarterly updates will be posted on this page.
This recording and the PowerPoint slides will be posted on the Electronic Visit Verification (EVV) quarterly updates page. Scroll down the webpage (about halfway) until you see the “Electronic Visit Verification (EVV)” header. You will also be able to find this information eventually on the EVV website as well.
Live-in caregivers
There is no modifier for live-in staff. Live-in caregivers must clock in and clock out using the EVV system at least once per workday. Caregivers may choose any time during the day to clock in and immediately clock out. The time of day does not matter as long as there is a clock in/clock out using the EVV system. The shifts may later be manually adjusted to reflect the number of hours worked and services provided during each shift.
For live-in staff who are properly identified in the EVV system as live-in/residing caregivers, it is expected that they will clock in and clock out using the EVV system at least once per workday. These shifts may be manually adjusted to reflect the actual number of hours worked and services provided during each shift. Alternatively, live-in caregivers may use the EVV system in real-time as any other caregiver would.
EVV policies
Read all EVV policies at the links below:
- Electronic visit verification (EVV) policy
- Electronic visit verification (EVV) live-in caregiver policy
- Electronic visit verification (EVV) device usage policy
- Electronic visit verification (EVV) verification methods policy .
Timesheets and billing
Paper timesheets may still be used in some cases. HHAX may not cover all the tasks involved in payroll data entry because EVV is designed to record only the time spent directly working with members. Additionally, the EVV system may not meet all statutory documentation requirements for all services your agency provides. Caregivers also have additional time for such activities as training, paperwork and troubleshooting that HHAX will not capture.
There are no changes to billing processes for EVV at this time. Providers will continue their current billing processes.
Billing is not required to go through EVV at this time. Billing and claims will be reviewed using a post payment review process to match claims to EVV visit data.
A telephone line is available for providers using the HHAeXchange system. If you are using HHAX and do not see this available, then you need to contact HHAX via their support portal.
No. Providers using third-party EVV systems must work with their third-party EVV vendor for IVR/telephony options and other device options.
We know providers, caregivers and members need time to learn the EVV system they selected and that it will take time for EVV to become routine. Your program may need to spend time and resources to ensure everyone understands and is trained on how to use your chosen EVV system. The state system from HHAeXchange offers two options for verifying EVV. Caregivers may use the mobile application available in numerous language options or may use the telephony option which is currently only available in English.
There are public resources available such as the Federal Lifeline benefit that people may qualify for to get a smart device. In some cases, both member and caregiver may qualify.
If the member or worker lack access to a phone, you may explore publicly available resources such as Lifeline, Telephone Assistance Plan (TAP) or the Affordable Connectivity Program (ACP). These are programs available that can either provide a wireless smart phone to the member or worker (i.e., something like Assurance wireless, or what you may have heard referred to as “Obama Phone” years ago), and discounts on phone and internet service through select providers. There are income requirements for these programs but often members and some caregivers qualify. More info is available from the Minnesota Commerce Department .
Safe at Home
Right now, if you're in the Safe at Home program and getting services or providing services, you won't need to use an EVV system. It doesn't matter if your provider picked a third-party system or the state-selected one – participants in the Safe at Home program are not required to use EVV.
Signatures are not required when using the EVV system; however, some services that require EVV have additional documentation and signature requirements that may be met outside of EVV. Review this page for more information.
In many cases, yes. Please review this page for the statutory requirements surrounding electronic signatures.
Shift adjustments/manual edits
Provider agencies may fix the EVV clock in or clock out with a manual shift adjustment in the EVV system on the administrative side. Providers should follow their existing internal processes for notifying workers when an adjustment has been made.
HHAX technical issues
Reach out to HHAX using the >HHAX Client Support Portal . Additional training and reference materials are available in your provider portal and LMS.
Managed care organizations (MCOs)
See the EVV website under the “Contact us” tab. If you are still unsure whom to contact, use the DSD Contact Form to reach out to the EVV team directly. DHS is developing a contact list specifying whom to reach out to at each MCO about their EVV process.
Provider agencies do not need to request that specific members be added to their portal from the MCOs. Each MCO follows an automated process of uploading members and authorizations into the EVV system when a prior authorization is required.
When a prior authorization is not required, it is the provider agency's responsibility to add the member and authorization to the system manually.
Not all services that require EVV require prior authorizations. The EVV requirements are determined based on the federal 21st Century Cures Act, which is the federal law requiring EVV.
September EVV quarterly session
Responses to questions raised at the Sept. 25, 2023, session:
Live-in caregivers must clock in and clock out into the EVV system at least once per workday. Live-in caregivers may use any of the EVV methods available to them, including the mobile application or interactive voice response (IVR). Caregivers may choose any time during the day to clock in and immediately clock out. The time of day does not matter as long as there is a clock in/clock out using the EVV system. The shifts may later be adjusted manually to reflect the number of hours worked and services provided during each shift.
Yes, shifts must be edited on a daily basis to reflect the actual time worked and services provided, to prevent potential overlap of a different service.
Shared care live-in staff will clock in and clock out the same as non-live-in staff. Each staff member must clock in and clock out separately (as two individual shifts), each single shift requires clock in and clock out.
The residing caregiver allows for documentation of the live-in caregiver within HHAeXchange. This is informational in the patient profile and EVV for these users and will follow the same methods as a non-live-in caregiver. For more information about live-in caregivers, see the Live-in caregiver policy .
IVR must be made from the client’s landline that is listed on their profile.
The caregiver code is the unique code assigned to each caregiver in the HHAX system. They are created automatically.
If you are a current user, HHAX is working to give providers lines. If you are new, you should receive it when you receive your credentials. It will be sent to the email used to complete the HHAX enrollment form.
When using IVR, if there is only one service authorized to the provider agency, the system will automatically associate the visit with the authorized service code. When there are two or more services authorized to the provider agency, the call will go to the call maintenance dashboard for the provider agency to associate the call with the accurate service codes and times.
You can use the IVR process guide to list out all the duties and share with your caregivers. You can access the process guide within the support center in your portal.
Assignment ID is only for the IVR verification method. The assignment ID can be found in the caregiver’s profile in HHAeXchange.
Yes. The IVR call in and call out must be made from the member's landline that’s on file which confirms you are at the location. See also the Device usage policy and the Verification methods policy .
DHS reduced the EVV geofence, which is a virtual perimeter around the home address of the member receiving services, from 500 miles to 500 feet from a member’s home effective Dec. 1, 2023. Provider agencies using EVV systems must select the “community” option when providing services or visits outside the geofence range. State-selected HHAeXchange users must check the community box in the mobile application. Third-party system users must work with their EVV vendor.
This was updated with the July 25 and 27 spec update . Search for "locationtype" to find details of optional community tags on visits outside the established geofence.
The specifications do not collect a geofence. As you can see in the current specification, the visit coordinates must be submitted. The geofence validation occurs in HHAX upon visit import. Third-party providers may note if a visit is conducted in the community by populating that field as outlined in the specifications. Providers using third-party EVV systems will continue to submit coordinates for their visit data. The specifications now include a field to insert a value when a visit occurs in the community and should not be subject to geofence validation in HHAX.
There is not a reason code required for visits outside the geofence; however, agencies have the option to tag the visit as a "community" visit to avoid rejection or other issues with the visit.
When the Community Visit checkbox is selected on the mobile app, the visit that is recorded will not be validated against the geofence. Providers should still instruct caregivers to record a clock in and clock out when in the community and selecting the Community Visit option so that these visits can be captured without validation to the home address. Community visits will still capture the GPS location at clock in and clock out.
Third-party EVV systems must maintain accountability to the state by submitting data that meets the state’s requirements to the HHAX data aggregator.
Members' addresses are sent from DHS MMIS to the provider's portal.
The 21st Century Cures Act requires that location of the service provided be collected as one of the six EVV data points. The geofence is a 500-foot perimeter around the person's home address that identifies visits as taking place in the home. The HHAeXchange system has a “community visit” checkbox that allows caregivers to acknowledge they are clocking in or out from a location greater than 500 feet from the person’s home. When the provider identifies the visit as a community visit, this enables the visit not to log a GPS or location error that must be resolved on the administrative side by the provider agency.
At this time, claims are not submitted via the EVV system and EVV data or errors will not cause any claim denials.
GPS location data is captured at the clock in and clock out of the visit. During the visit, caregivers do not need to make additional clock in/out (known as EVV calls) when changing locations. There is no GPS tracking or location requirements during a service visit.
The caregiver has the ability to leave a note in the mobile app when clocking out and can view how far they are from the member's address in the mobile app. Provider agencies can also add a note on the visit through the call dashboard in their provider portal.
HHAX technical questions
Submit a support request to HHAeXchange through their support portal here: Client Support Portal . After you reach out to HHAX with your question, you will receive a ticket number. If the problem still exists or if your question was not answered, use the DSD Contact Form . Select “PCA and EVV questions” in the drop-down menu, and then select “EVV policy and questions”; your questions will be routed to the EVV team. Include your HHAX ticket number. We cannot elevate your question until you have reached out to HHAX first and received a ticket number.
Submit your question to HHAeXchange through their Client Support Portal .
No. All password resets and new passwords expire after 12 hours. When requesting a new account or password, be aware of this limitation and make sure you are able to access email in a timely manner. If you need an additional password reset or other assistance, submit a support request to HHAeXchange through their Client Support Portal .
You can add a second and third address straight from the member's profile within the HHAX system.
The HHAeXchange EVV system offers two EVV verification methods, the mobile application and IVR. Additional verification methods might be available for provider agencies using third-party EVV systems. Providers choosing these third-party systems will need to work with their vendor to determine which options are available to them.
With HHAX, you can clock in and clock out as an unscheduled visit in the community.
Yes, providers are able to input a TEMP authorization into the system if needed. This is true for all provider portals: FMS, CFSS, Waiver and HHS.
When using the mobile app, caregivers can select the service code for the service they are providing, or they can use scheduled visits and the service code would be locked and all they must do is clock in/out. If the caregiver selects the wrong code, the provider agency will need to go back and update later to the correct service.
Provider portals are automatically updated from MMIS with member information through the HHAX EVV Aggregator.
If caregivers are helping a member in the community, they should use the "community" checkbox.
DHS has not yet released policy for these instances. As this time, please focus on onboarding and having your workers and members who have service authorizations use EVV.
The responsibility of agencies is crucial in preventing any misuse of the community visit option. Caregivers must adhere to the requirement of clocking in and out within a 500-foot radius of the member's residential address. While we encourage the use of the "community" checkbox for accurate documentation during community-based support, it's essential that agencies monitor and ensure its correct use. The community checkbox should only be employed when caregivers are genuinely engaged in community-based member support. It is not intended as a means to circumvent the mandatory clock-in and clock-out procedure within the 500-foot geofence. Agencies should actively monitor and ensure that caregivers are following the rules to maintain compliance and avoid abuse and fraud.
Note that location data is still captured at the clock in and clock of out an EVV visit. Clocking in early or in unallowable locations is considered fraud. Provider agencies are able to check the location of the clock in and clock out to ensure accuracy of location data and maintaining program integrity.
The type of service, individual receiving the service, date of the service, location of the service, individual providing the service and the time that the service begins and ends. For more information, see the Electronic visit verification webpage and Electronic visit verification (EVV) in the Community-Based Services Manual .
DHS has not yet released policy on this specific topic. If your agency is using HHAeXchange, you have access to the services portal which can help with keeping a record of these shift adjustments.
Shift adjustments and edits should be limited whenever possible, but we understand there are circumstances in which edits will be unavoidable. DHS is not enforcing compliance that will result in claim denials or reversals. DHS is developing compliance policies as we move toward full implementation of EVV.
DHS recognizes that providers, caregivers and members need time to learn to use EVV and that it will take time for it to become routine. Until a compliance requirement is published, DHS will be monitoring usage and use to ensure providers are prepared before being required to meet compliance thresholds. DHS is required to report quarterly usage to the federal Centers for Medicare & Medicaid Services (CMS).
For live-in staff who are properly identified in the EVV system as live-in/residing caregivers, we expect providers to adjust shifts manually to reflect the number of hours worked and services provided during each shift. Or they can clock in and clock out in real time.
Yes, if a member has a responsible party, they may log in and propose shift adjustments in the services portal.
EVV third-party vendor
If you are using a third-party vendor, you should not need to log into HHAX.
Providers using third-party EVV systems do not need to manually manage visits in the HHAX portal. HHAX will only receive approved visits from third-party EVV systems. Any rejected visits from a third party will reject in their source system for provider agencies to manage and resend.
Third-party providers can use the HHAX EVV API which can import visits in real-time. EVV does not need to be sent to HHAX for import on a real-time basis for purposes of the daily clock in and out activities as long as those occur in the provider's third-party EVV system.
HHAX services portal
Service Portal Management is under the admin tab in your main HHAX portal.
The services portal is an optional feature that provider agencies may choose to allow members and caregivers to review, adjust, approve or reject recorded shifts.
Not all EVV services require shift approval by the member. Only PCA services require the member/patient to approve shifts. The agency is not allowed to approve shifts for the patient. For more information, see PCA Documentation Requirements . For PCA services, if the patient does not have access to the patient service portal, the agency will need to find another way for the patient to approve shifts. This could be via a responsible party, continued use of paper time and activity documentation, or assisting the member in finding resources that enable them to access the services portal.
Visits are always viewable through the service portal. Visits that have not been approved by the member/responsible party or caregiver are viewable to the provider agency with a flag “missing service portal approval.” Once the shifts are approved in the services portal, the status changes to “approved locked.” Provider agencies can search for visits using the above statuses.
Members and caregivers/responsible parties can review previously approved shifts by filtering through the “approved locked” shifts.
Signatures/approvals
Signatures are not required when using the EVV system; however, if you are providing PCA services, you have two options to meet the time and activity documentation requirements for caregivers and members:
For caregiver signature/acknowledgement you have two options:
- [current process] The caregiver will clock in and clock out using your program’s EVV system as usual and additionally they will sign a time and activity documentation on a paper format.
- Your program may choose to use the Service Portal in the HHAX system. There is no actual handwritten signature required in the HHAX system. Before staff clock out, it’s a button to push for acknowledgement. When a staff member clocks out, a Tennessen warning will pop up for staff to acknowledge before allowing staff to clock out. That acknowledgement counts as the staff’s signature.
For member signatures/approvals, you have two options:
- The member can sign a time and activity documentation in a paper format. They could potentially use the DHS PCA provider time and activity documentation .
- Your program may choose to use the Service Portal in the HHAX system. A member should never interact with the HHAX app on a staff member’s phone. For member/responsible party approval of a shift, the member/responsible party will receive an email to click a button to approve shifts. The member/responsible party can approve shifts by checking their email anytime and approve each shift at their convenience.
In-scope services
Yes, H2014:UC:U3 is a service code in-scope for EVV.
See also the EVV website under the Required services tab or this detailed list of required services for EVV .
HHAX as a free system is not intended to be a timekeeping or payroll system. DHS is exploring with HHAX what additional features and support to create efficiencies will be available.
Internet and cell phone resources
If the member or worker lack access to a phone, you may explore publicly available resources such as Lifeline, Telephone Assistance Plan (TAP) or the Affordable Connectivity Program (ACP). These are programs available that can either provide a wireless smart phone to the member or worker (i.e., something like Assurance wireless, or what you may have heard referred to as “Obama Phone” years ago), and discounts on phone and internet service through select providers. There are income requirements for these programs but often members and some caregivers can qualify. The state Commerce Department has published more information about these programs.
Electronic visit verification is a system for verifying, through an electronic verification system, that services have been provided. Section 12006(a) of the federal 21st Century Cures Act (PDF) requires states to use EVV for all Medicaid personal care services, including some waiver services, and home health services. Providers of affected services must begin to use EVV in collaboration with the Minnesota Department of Human Services. DHS will provide guidance and policies to provider agencies to ensure the requirements of the 21 st Century Cures Act are met. Providers may create additional EVV policies but they must conform to DHS EVV requirements.
The EVV system must verify that home or community-based service visits occur by collecting six points of data electronically:
- Type of service performed
- Who received the service
- Date of service
- Location of service delivery
- Who provided the service
- When the service begins and ends.
In Minnesota, personal care services that will be required to use EVV are:
- Consumer Directed Community Supports (CDCS) direct support
- Consumer Support Grant (CSG) direct support
- Crisis respite
- Homemaker-assistance with personal cares
- Independent community living support (in-person)
- Individualized home supports, with and without training (in-person)
- Night supervision
- Personal care assistance
- Respite care services (in-home).
In Minnesota, home health services that will be required to use EVV are:
- Home health aide
- In-home occupational therapy
- In-home physical therapy
- In-home respiratory therapy
- In-home speech and language therapy
- Skilled nurse visits
- Direct skilled nurse visits.
Additional services might be subject to EVV. If DHS adds additional services, we will communicate these changes via eList and website updates.
For a list of services that require EVV, see the Electronic visit verification webpage under the Required services tab or this detailed list of required services for EVV .
Yes. EVV is required for all mandated services, regardless of where services start and end.
Providers may choose to use their EVV system for other services not in-scope, but only in-scope services will be reported to the state-selected EVV system from HHAeXchange.
Live-in caregivers are exempt from some EVV requirements, according to federal guidance. Live-in caregivers must enter the following required information into the EVV system at least once per day:
- Person who received the service
- Date of the service
- Location of the service delivery
- Person who provided the service
DHS offers the option for provider agencies to have live-in caregivers will interact with the EVV system on a daily basis instead of in real-time. Live-in caregivers must clock-in and clock-out into the EVV system at least once per workday using any of the EVV methods available to them. Caregivers may choose anytime during the day to clock-in and immediately clock-out. The time of day does not matter as long as there is a clock in/clock out using the EVV system. The shifts can later be manually adjusted to reflect the number of hours worked and services provided during each shift.
Provider agencies can choose to require live-in caregivers to interact with the EVV system in real time.
See also CBSM – EVV live-in caregiver policy .
At this time, participants in the Safe at Home program should not use EVV in any capacity. DHS is working to determine the appropriate options to ensure information remains confidential.
No, EVV does not affect the services a person is authorized to receive.
Minnesota's system
DHS has selected a hybrid EVV model. Providers may choose the state-provided EVV system, or a third-party EVV system that meets state requirements. Third-party systems must meet the requirements of the 21 st Century Cures Act and maintain accountability to the state by submitting data to the state’s system.
DHS has selected HHAeXchange (HHAX) to provide the electronic visit verification (EVV) system for Minnesota. The contract was finalized on May 25, 2021. For more information about HHAeXchange, visit the HHAeXchange Minnesota Provider Information Center .
DHS will not charge a fee to providers to use the state-selected EVV system. However, we understand that providers may need to spend time and resources to make a change this large and to comply with state and federal requirements.
Providers who choose to use a third-party EVV system will pay for their chosen system.
As of Oct. 16, 2023, all Minnesota providers are to use EVV. Providers of services in scope need to complete the EVV onboarding process and begin using their EVV system now. For a list of services that require EVV, see the EVV website under the Required services tab or this detailed list of required services for EVV .
- Phase 1 : Financial management services (FMS) for personal care services. Launched June 20, 2022.
- Phase 2 : Remaining personal care services. Launched Dec. 12, 2022.
- Phase 3 : Managed care organizations (MCOs) for personal care services. Launched June 5, 2023.
- Phase 4 : Home health services. Launched Oct. 16, 2023. All home health service providers launched, regardless of payer.
We know providers, caregivers and members need time to learn the EVV system they selected and that it will take time for EVV to become routine. We are not enforcing compliance that will result in claim denials or reversals in 2023 and into the beginning of 2024. We will monitor EVV use until we publish compliance requirements to ensure you are prepared to meet them.
We are required to report EVV use to the Centers for Medicare & Medicaid Services quarterly and identify providers who are not using an EVV system. We will provide technical assistance to providers identified in the reports as we move toward compliance requirements.
The Department of Human Services is using what we learned from the first two electronic visit verification launches to help develop policies and guidance for providers so they are able to comply with state and federal EVV requirements.
Providers of services that have launched for EVV services in the initial phases of the system launch need to complete the EVV onboarding process and begin using their EVV system now.
We know providers, caregivers and members need time to learn the EVV system they selected and that it will take time for EVV to become routine. We are not enforcing compliance that will result in claim denials or reversals in 2023. We will monitor EVV use until we publish compliance requirements to ensure you are prepared to meet them.
DHS recommends caregivers use the mobile application to verify EVV visits within the state EVV system, HHAeXchange (HHAX), whenever possible. DHS and HHAX offer a secondary verification method for EVV using a telephone system known as interactive voice response (IVR).
Providers who use a third-party EVV system will need to work with their vendor on device options for EVV. DHS does not oversee devices for third-party system users. Providers may use what works best for their organization as long as it captures the required EVV data.
DHS does not provide any devices for EVV. There are public resources available, such as the Federal Lifeline benefit that people might qualify for to get a smart device. In some cases, both member and caregiver might qualify.
If the member or worker lacks access to a phone, they may explore publicly available resources such as Lifeline, Telephone Assistance Plan (TAP) or the Affordable Connectivity Program (ACP). These are programs that can either provide a wireless smart phone to the member or worker, or discounts on phone and internet service through select providers. The state Commerce Department has published more information about these programs.
DHS understands there are barriers for some people to use the EVV system. The HHAX mobile application is available in multiple languages to meet the needs of Minnesotans. In addition, the HHAX mobile application uses visuals which make it easy to use even when language is an issue.
Available languages include:
- English (North America)
- Spanish (Latin America)
- French (European)
- Chinese (Traditional)
- Haitian Creole
- Karen (Burmese)
Note: Other languages may be added in future releases.
HHAX training materials are available in Spanish, Hmong, Somali, Vietnamese and Russian.
Providers who use a third-party EVV system will need to work with their vendor to meet the language needs of the people they serve and their caregivers.
At this time, there is no change to how providers bill for services provided. Providers will continue to use the billing processes they use now. DHS continues to explore billing enhancements for the HHAX system.
Providers will need to fill out an updated Provider Enrollment Form and create a ticket through the HHAeXchange support portal to notify HHAX and DHS of the change.
- Provider Enrollment Survey for PCA and Waiver: Provider Enrollment Form
- Provider Enrollment Survey for Home Health: Provider Enrollment Form
Providers who switch EVV systems will need to follow the steps to either join the HHAX system or to connect their third-party system.
A schedule is not required to confirm EVV-compliant visits. There is a scheduling feature in the HHAX system that providers may use if they choose.
In Minnesota, EVV is required for both home and community visits. DHS has established a 500-foot, or about 1.5 football fields in length, geofence around a person’s home address. This virtual perimeter identifies where the visit took place. For visits occurring outside the 500-foot geofence, there is a checkbox in the HHAeXchange system to acknowledge that the caregiver is outside of the geofence and notes the visit as a community visit.
Providers using third-party EVV systems will need to work with their vendors to configure their geofence to 500 feet and actions for visits outside the geofence.
Signatures are an optional component of the EVV system. Not all EVV services require shift approval by the member, but providers may choose to require signatures for services.
If choosing to require signatures in the EVV system, providers must ensure that their EVV system meets the following criteria for electronic signatures as determine by Minnesota Statutes 325L.02(h) and 325L.09:
- "Electronic signature" means an electronic sound, symbol or process attached to or logically associated with a record and executed or adopted by a person with the intent to sign the record.
- An electronic signature must be attributable to a person. An electronic signature is attributable to a person if it was the act of the person, which can be shown from the context and surrounding circumstances at the time of its creation, execution or adoption.
You should know that some service providers might need extra documentation for the services they offer. These documentation requirements might not be covered by the EVV system. For questions about specific programmatic documentation and signature requirements, contact the program policy or licensing area at DHS directly.
HHAX system users
Providers must complete the HHAX provider enrollment survey for the services they provide to begin the process. The email used to complete the survey will be the email used to receive communication from HHAX. Then users will review the information sessions posted to the HHAX Minnesota Provider Information Center .
- Personal care provider enrollment survey
- Home health provider enrollment survey .
Once providers complete the form, they will receive their learning management system credentials typically within three to five days. Check the email used to complete the form.
Once providers complete the survey, they will receive their HHAX system portal credentials in the email used to complete the survey. The admin user at your agency will be responsible for adding all additional staff to HHAX.
Access the HHAX system portal via a web browser, available on a phone, tablet or computer.
For services that have prior authorizations, HHAX connects with DHS for member and authorization data from the MMIS system. Members are then connected to their provider portal.
For services that do not require prior authorization, providers should contact their payer directly for processes and procedures. In the HHAeXchange system, services not requiring a prior authorization will need to be manually entered into the system by the provider agency.
HHAX creates a single provider portal for all providers based on the provider tax ID. HHAX then creates service type-specific offices once the provider has submitted the Provider Enrollment Form and has provided their UMPI/NPI numbers. There are potentially four different offices a provider may have in their portal:
- CFSS (includes PCA services)
- Home Health.
For specific questions about setting up a specific office in your portal, use the HHAX Client Support Portal .
Once providers have received portal credentials, they can begin entering caregiver information into the EVV system. Please review the guides provided by HHAX on the process to enter caregiver information and connecting them to members.
The HHAX mobile app has an offline mode for cases where cell or internet service is not available. Once cell service or internet service reconnects the information will automatically upload into the application.
Third-party EVV system users
The HHAX aggregator is the name of the system for collecting EVV data from providers and members and reporting it to DHS. Providers should review the following specifications and requirements on the HHAX Minnesota Provider Information Center webpage under the EDI tab before beginning the process to connect to the aggregator:
- Business requirements: Business Requirements for Third Party EVV Data Aggregation MN
- Technical specification document: HHAeXchange EVV API Technical Specifications MN
Providers must complete the Provider Enrollment form to indicate they will be using a third-party EVV system and the name of the system they will be connecting to the data collector. The email used to complete the survey will be the email used to receive communication from HHAX.
Once you complete the survey, use the HHAX Client Support Portal to create a ticket. Select the box titled “Provider EDI Integration.” HHAX will send providers an attestation form they will need to complete before the connection can begin.
- Review the information session recordings found on the HHAX Minnesota Provider Information Center.
- Review the EDI webinar found on the EDI process tab on the HHAX Minnesota Provider Information Center.
Providers will begin testing in the testing environment with their third-party vendor and HHAX. Once testing is successful, agencies will receive their production credentials.
Providers then can begin sending data to HHAX. Providers need to review any rejections they receive and correct them in a timely manner.
Once providers complete the provider enrollment survey, they will receive their HHAX system portal credentials in the email used to complete the survey. The admin user at your agency will be responsible for adding all additional staff into HHAX.
Providers will have access to the learning management system (LMS) where they can access modules to help them navigate the system. Providers will also have access to process guides and job aides in their provider portals.
Providers who use a third-party EVV system need to work with their vendor for training in their EVV system. Third-party EVV system providers will have access to the HHAX LMS to complete the EDI module. They will have access to the other modules in LMS to use for reference when reviewing data.
Providers will receive their LMS credentials within three to five business days of completing the provider enrollment survey.
Providers are responsible for training and ensuring caregivers, members and responsible parties feel comfortable with the system.
Providers who use HHAeXchange will have access to tools and materials to train caregivers, members and responsible parties on how to use the system.
Providers who use a third-party system will need to work with their vendor on how to train caregivers, members and responsible parties.
Training material provided by HHAX are available in several languages, including Hmong, Russian, Somali, Vietnamese and Spanish. Providers who use a third-party EVV system will need to work with their vendor to meet the language needs of their organization.
Continued engagement
DHS is committed to engaging providers, recipients, direct workers and other interested community members as we begin to use EVV. To receive announcements about engagement sessions, sign up for eList announcements on the Electronic visit verification webpage under the Public input tab.
Visit the Electronic visit verification webpage where you can see the latest updates. To receive notification of updates, select the Contact us tab and scroll to the end of the page and sign up using your email. You may then update the subscription to select “General stakeholder news: disability services.”
- Policy-related questions
- DHS-specific questions
- Electronic visit verification webpage
- HHAX system users: [email protected]
- Phone: 855-573-1521
- System use/training questions
- Onboarding into the system
- All issues directly related to the system or technical questions
- HHAX Minnesota Provider Information Center
Members and caregivers should contact their provider agency with questions or concerns they have about EVV.

An official website of the United States government Here’s how you know
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock A locked padlock ) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.
Electronic Visit Verification Outcomes-Based Certification
Related resources.
Informational Bulletin: Outcomes-based Certification for Electronic Visit Verification (EVV) Systems (PDF 184.96 KB)
EVV Programmatic Resources
Section 1903(l) of the Social Security Act, as added by section 12006 of the Cures Act (Pub. L. No. 114-255) and further amended by Public Law No. 115-222, stipulates that states will be subject to a reduction in Federal Medical Assistance Percentages (FMAP) if they do not implement Electronic Visit Verification (EVV) for personal care services by January 1, 2020, and for home healthcare services by January 1, 2023, absent a one-year extension based on the Centers for Medicare & Medicaid Services (CMS) approval of a state’s Good Faith Effort application. While the Cures Act does not require states to have their EVV systems or data aggregation solutions certified for federal financial participation (FFP) to avoid FMAP reduction, it does allow states to apply for FFP for EVV systems. If a state applies for FFP under the Advance Planning Document process, its EVV solution will need to be certified.
CMS has developed a streamlined, outcomes-based approach to EVV certification. This approach focuses on achieving business outcomes embodied in the Cures Act and is intended to reduce the certification burden on states. In doing so, CMS aims to ensure that systems receiving FFP are meeting the business needs of states and of CMS. EVV certification is structured around the following elements:
- Outcome statements. These describe the desired results once the system is implemented. CMS-provided outcomes are based on the Cures Act.
- Evaluation criteria and required evidence. These correspond to outcome statements and are used by a state and CMS to evaluate the system’s functionality and its compliance with laws, regulations, and industry good practices.
- Key performance indicators (KPIs). These metrics support the outcome statements and are used to track the performance of the system over time.
Compared to the process found in the Medicaid Enterprise Certification Toolkit (MECT), this process for EVV certification is streamlined in the following ways:
- Reduced Certification Evaluation Criteria. The number of certification evaluation criteria is reduced from 146 to 11.
- Streamlined Reviews. States undergo an Operational Readiness Review before the system goes live. At least six months later, a Certification Review is conducted. Project Initiation Milestone Reviews are eliminated.
- Introduced Quarterly KPI Reporting. The state reports on KPIs at least once after the Operational Readiness Review and then quarterly after certification. Quarterly reporting is required for as long as a state continues to receive enhanced funding for operations and maintenance.
- Reduced Artifacts List. Except for the certification request letter and system acceptance letter, the state does not need to prepare artifacts listed in MECT Appendix B, nor does it need to prepare a Project Partnership Understanding.
EVV Certification Version 1.0
CMS released EVV Certification Version 1.0:
EVV Certification 1.0 (ZIP 1.6 MB)
- 00 EVV Certification 1.0 EVV Release Notes
- 01 EVV Certification 1.0 EVV Guidance
- 02 EVV Certification 1.0 EVV Evaluation Criteria and KPIs
- 03 EVV Certification 1.0 EVV Intake Form
Learn More About Our Platform
Caregiver management.
Caregiver Satisfaction Survey
- Custom Forms
- Custom Reporting
Electronic Visit Verification (EVV)
Client Relations
- Client + Family Portals
- Hospitalizations
- Payment Processing
Point of Care
- Medication Reminders
- Visit Insights
Administration
Business Intelligence
Two-Way Chat
By Agency Size
- Enterprise Agencies (1,000+ Clients)
- Medium to Large Agencies (30-1,000 Clients)
- Small Agencies (Up to 30 Clients)
- Office Managers
- Sales + Marketing
- Clients + Families
By Payer Source
- Veteran Affairs
- Private Pay

Bridging the Gap: Overcoming Challenges in Online Home Care Software Adoption

How to Expand Person-Centered Care: Strategies and Insights

How to Prioritize an Effortless Experience for Your Caregivers When Selecting Home Care Software
More resources.
- Caregiver Resources
- Case Studies & Testimonials
- Glossary of Terms
- Home Care Software Reviews
- Integrations Marketplace
Security at AxisCare
- White Papers & Tip Sheets
In a world where technology often takes precedence over people, we’ve chosen a different path – one that combines cutting-edge innovation with genuine care.
Press Releases
Stay up-to-date with the latest press releases and news coverage about AxisCare.
If you’re ready to grow your career while making a difference in the lives of seniors around the world, you’ve come to the right place.
- (800) 930-7201
- [email protected]
- 1105 Wooded Acres Dr, #300 Waco, TX 76710
Understanding EVV: The How, When, & Why of Electronic Visit Verification
Introduction.
Being a home health care provider is nothing like working a traditional nine-to-five. Caregivers are on the road for most of the day, jumping between appointments based on a carefully coordinated schedule.
With so many variables at play, maintaining time sheets and ensuring accountability can be challenging – which is why the industry utilizes Electronic Visit Verification (EVV).
What is Electronic Visit Verification (EVV)?
What is EVV? EVV software is utilized by home care agencies and their caregivers to electronically record the start and end times of home-based healthcare services. The 21st Century Cures Act mandates the use of EVV for health care provided at home or in the community, aiming to prevent fraud by verifying that the services billed for were actually rendered.
The Evolution of EVV
Early manual systems (pre-2000).
Before the new millennium, EVV was still in its infancy. Early systems relied mostly on analog inputs like paper-based documentation and manual reporting.
Telephony-Based Solutions (Early 2000s)
In the early 00s, change came calling. Caregivers could use landlines or mobile phones to clock in and out of visits, which helped automate the verification process.
Mobile Technology Integration (Mid-2000s)
A few years later, caregivers began using smartphones and more advanced mobile devices to log their visits, allowing for increased flexibility and real-time data transmission during visits.
Regulatory Mandates (2010s)
The 21st Century Cures Act was signed into law in December 2016, mandating the use of EVV for Medicaid-funded personal care services and home health care services.
Comprehensive EVV Solutions (2015-2020)
EVV solutions began integrating complementary technologies like caregiver mobile apps, including GPS tracking, electronic signatures, and digital documentation, creating more comprehensive and powerful toolkits.
How Does EVV Work?
These days, caregivers typically use smartphones and tablets to engage with EVV solutions and track their visits while on the move. Here’s what a typical workflow looks like:
Initiating a Visit (Check-In)
Caregivers use their devices to log into their EVV-enabled point-of-care software . This creates an exact timestamp to mark the start of the at-home session.
Authentication & Identification
Caregivers enter a password, PIN, or use biometric verification such as a fingerprint scan or Face ID on their device to confirm their identity.
Location Tracking
EVV uses GPS technology to track and record caregivers’ locations, providing real-time information about their presence at the designated service location.
Task Documentation
Caregivers record every task performed during their visit, including specific care details like medications administered and client notes.
Integration With EHR
EVV systems typically integrate with Electronic Health Records (EHR), creating a link between at-home care documentation and the client’s overall healthcare record.
Compliance Checks
EVV systems routinely perform compliance checks to ensure that the care provided meets regulatory requirements for uses such as Medicaid billing and that the visit adheres to the applicable care plan.
Caregiver Check-Out
Once a visit is complete, caregivers clock out in the same way they started the session, marking the exact end time and confirming all necessary services have been rendered.
Real-Time Reporting
EVV systems generate reports that provide immediate access to visit data, helping agencies monitor, bill, and verify caregiver activities.
Regulatory Overview of EVV
The 21st century cures act & evv.
The 21st Century Cures Act was written into law in 2016 to mandate the use of EVV. Its goal is to enhance caregiver accountability, reduce fraud, and improve the overall quality of care using technology to track and verify services rendered.
Service Type
These regulations apply to Medicaid-funded personal and health care services delivered at home and in community-based settings. For Medicaid billing in most states , the following must be captured in order for home care agencies to receive compensation for the visit being completed:
- Individual Receiving the Service
- Date of Service
- Location of Service Delivery
- Individual Providing Services
- Beginning and End Times of Service
State-Specific Mandates for EVV
While the Cures Act and CARES Act legislate at the federal level, some states have implemented additional requirements for EVV.
Open Model State: In an Open Model State, Medicaid providers can choose from a variety of approved EVV systems that meet the state’s requirements. This approach allows for a more diverse and adaptable landscape for EVV solutions, promoting innovation and accommodating different healthcare providers’ preferences.
Closed Model States: Closed Model States take a more centralized approach. They will typically choose a single EVV system to be used by all Medicaid providers in that state or create one themselves. This aims to simplify implementation, facilitate standardized reporting, and keep things consistent across the state’s healthcare system.
Understanding Aggregators: An EVV aggregator is a third-party platform that collects and verifies information from state-level Medicaid data sources. This information includes services rendered, billing claims, and client records, which are transmitted to the specific payer.
Applications of EVV in Healthcare
It may be clear by now that EVV is far more than just a tool for clocking in and out of a client visit. This technology can be used in countless ways across the entire care ecosystem, all of which contribute to a more efficient and productive workflow.
Medicaid-Funded Personal Care Services
As previously mentioned, EVV is the standard for Medicaid-funded care environments, ensuring accurate tracking and verification as mandated by federal and state legislation.
Home & Community-Based Services (HCBS)
EVV helps community-based caregivers manage and document a wide range of services, enabling them to coordinate care and preserve accountability outside of a traditional healthcare setting.
Remote Patient Monitoring
EVV can also be used to track and verify caregiver interactions for services administered virtually or remotely – an increasingly valuable feature as telehealth continues to become more prevalent in the home health care industry.
Chronic Care Management
EVV helps monitor and document recurring healthcare services (both in-person and remote), ensuring clients with chronic conditions receive consistent and timely care.
Hospitalization Care
After a hospitalization occurs, hybrid programs like transitional care and hospital-at-home initiatives can be tracked using EVV technology.
Hospice Care
EVV can be used to log hospice care being provided at home, ensuring comfort and support for individuals who are navigating the final stages of life.
Benefits of EVV Compliance
Aside from remaining in good standing with government regulations, there are plenty of ways that EVV usage benefits agencies and providers. Like most leaps toward automation, perks include a boost in efficiency and less busy work for employees. EVV also lends a hand in creating a heightened level of trust between agencies and their clients since they know services will be rendered and documented.
Improved Productivity
By automating routine tasks that used to be completed manually – like time tracking and reporting – EVV gives caregivers more time and energy to focus on delivering care.
Faster Payments
EVV can accelerate the billing cycle by immediately verifying and logging visit information, which, in turn, leads to faster reimbursements for healthcare providers.
Better Client Outcomes
EVV helps agencies and other providers adhere to care plans and deliver timely care by amalgamating critical information in a single spot, all in real-time.
Reduced Errors & Fraud
As a system designed to increase transparency and accountability, EVV is the best way to ensure caregivers track their services in a fair and accurate way while verifying that resources are used efficiently.
Improved Access of Information
Digitizing and centralizing client data makes it easy for all relevant stakeholders to retrieve client records, care plans, and visit details. In turn, this contributes to more informed decision-making.
Enhanced Caregiver Experience
The use of EVV and mobile apps offers caregivers a more seamless visit experience by eliminating administrative burdens, improving communication with their employer, and ensuring timely pay as their clock-in and out times are documented with ease digitally.
Considerations for Implementation
Data-driven insights risk mitigation.
EVV mitigates risk by facilitating compliance with regulations, reducing billing discrepancies, and increasing transparency. This helps agencies and providers avoid legal and financial issues associated with non-compliance or documentation errors.
Understand State Requirements
As we mentioned above, different states may have their own set of regulations governing the use of EVV, like the open versus closed model framework. Conduct a thorough assessment to make sure you understand your specific local requirements so you can remain on the right side of the law.
Compliance With EVV Regulations
No matter how you use your EVV solution, it will need to strictly adhere to both federal and state EVV regulations , such as those put forth in the 21st Century Cures Act. By remaining in compliance with these rules, you can avoid potential penalties and maintain eligibility for critical Medicaid funding.
Verify Software Features
Get to know your EVV solution’s features in-depth to make sure they align with your needs. Key synergies to look out for include real-time reporting, seamless integration with Electronic Health Records (EHR), and compatibility with your existing home care software and tech suite.
Provide Training & Support
Every time you onboard a new software, you’ll need to teach stakeholders how to use it. Establishing an EVV training program for caregivers and staff is a must for successful adoption, coupled with ongoing support mechanisms that will help them solve future issues as they arise.
Before AxisCare, CDM Caregiving Services was using a software provider that wasn’t on top of impending EVV compliance deadlines. With CDM’s client base being 90% Medicaid, the pressure was on to find a provider that took their concerns seriously and had compliance solutions in place.
CDM chose AxisCare for our user-friendly EVV-compliant Mobile App and our eagerness to understand their state’s EVV complexities. Now, CDM not only uses AxisCare to track and bill Medicaid clients but also to manage and run the adult day center where seniors in their community can come for physical therapy, companionship, and socialization.
Thanks to EVV, home health care has come a long way from manual note-taking and documentation systems. Agencies have lots to gain from implementing an EVV-enabled solution, from drastically reducing their administrative burden to avoiding human error and boosting accountability.
Implementing your own EVV solution requires a deep understanding of state requirements and evolving compliance features – so nothing compares to collaborating with an industry pro like AxisCare. Book a demo with one of our experts to learn everything you need to know about our EVV integrations, our app, and other useful features for home care agencies.
References and Resources:
- EVV Software for Home Care
- 21st Century Cures Act
- Point of Care Software
- Medications Administered
- Medicaid Billing
- Seamless Visit Experience
- State EVV Regulations
- EVV Training
- CDM Caregiving Services
- EVV-Compliant Mobile App
- 1105 Wooded Acres Dr, #300 Waco, TX 76710
Platform Features
Caregiver Mobile App
Case Studies & Testimonials
- Home Health Care Software
- Private Duty Home Care Software
White Papers & Tip Sheets
Privacy Policy
- Terms & Conditions
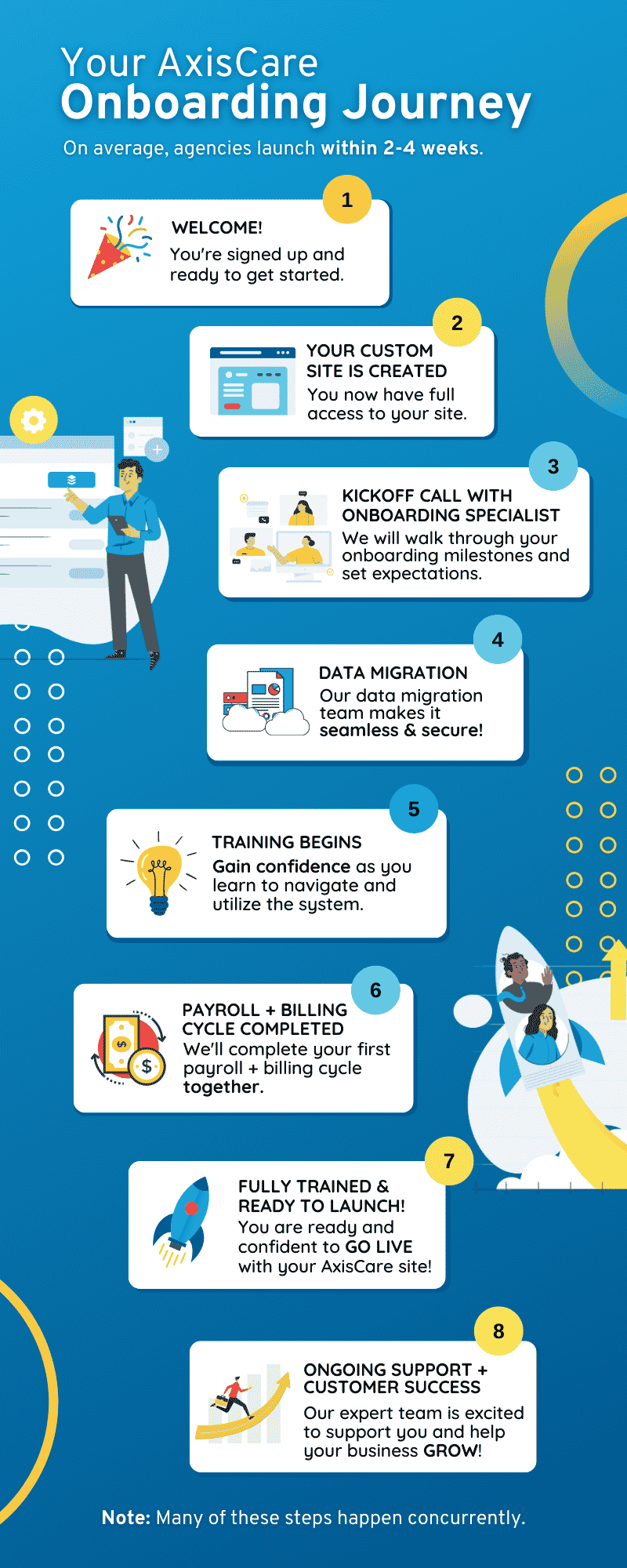
Don’t settle for average software onboarding. Experience the AxisCare difference.
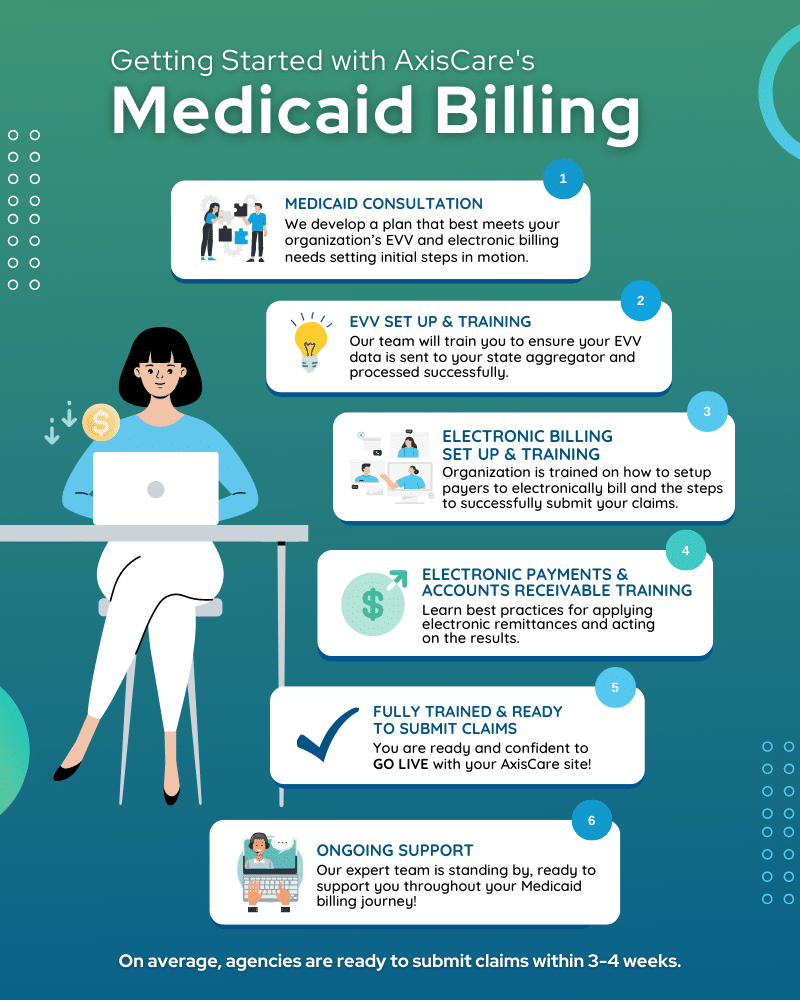
IMAGES
VIDEO
COMMENTS
Electronic Visit Verification (EVV) Section 12006 (a) of the 21st Century Cures Act mandates that states implement EVV for all Medicaid personal care services (PCS) and home health services (HHCS) that require an in-home visit by a provider. This applies to PCS provided under sections 1905 (a) (24), 1915 (c), 1915 (i), 1915 (j), 1915 (k), and ...
A state will demonstrate its EVV solution's achievement of these outcomes through evaluation criteria and KPIs. There are 11 evaluation criteria and five KPIs (see Figure 1). The evaluation criteria can be found in 02 EVV Certification 1.0 Evaluation Criteria and KPIs. Figure 1. Outcomes, Key Performance Indicators, and Criteria.
for a streamlined, outcomes-based approach to certify Electronic Visit Verification (EVV) systems used for all Medicaid personal care services and home health services requiring an in-home visit by a provider. Per section 1903(l) of the Social Security Act (the Act), as added by the 21st Century
The 21st Century Cures Act included a federal mandate requiring healthcare providers to use electronic visit verification, or EVV. Individual states continue to roll out their solutions as only a small number managed to meet the January 1, 2020 deadline. As of January 1, 2023, all agencies must have implemented EVV, including home healthcare companies.
This table lists each state or territory's compliance status with Electronic Visit Verification (EVV) requirements as of January 1, 2024 for home health care services. States and territories were required to self-report their EVV implementation status using a web-based survey, which the Centers for Medicare & Medicaid Services (CMS) used to determine compliance with the EVV requirements ...
This table lists each state or territory's compliance status with Electronic Visit Verification (EVV) requirements as of January 1, 2021 for personal care services. States and territories were required to self-report their EVV implementation status using a web-based survey, which the Centers for Medicare & Medicaid Services (CMS) used to determine compliance with the EVV requirements ...
Electronic Visit Verification (EVV) Phase I. Electronic visit verification (EVV) is an electronic-based system that collects information through a secure website, a mobile application ("app") or a telephone. Federal law, Subsection l of Section 1903 of the Social Security Act (42 U.S.C. 1396b) , requires all states to implement EVV for ...
The Centers for Medicare and Medicaid Services (CMS) has released new guidance, including a new Frequently Asked Questions document, on the mandate that states require electronic visit verification (EVV) for personal care services by January 1, 2020 and for home health care services by January 1, 2023.
Our report, Electronic Visit Verification: The Weight of Surveillance and the Fracturing of Care, explores how the public sector adoption of EVV technology has ignored the needs of marginalized communities and has led to tangible harms. The mandatory rollout of EVV technology has eroded critical supports for people with
This document serves as an informational reference for stakeholders participating in the NY Medicaid Electronic Visit Verification (EVV) Program. Although reasonable effort has been made to assure the accuracy of the information within these pages at the time of posting, it is the responsibility of each provider and fiscal intermediary to ...
Electronic Visit Verification . EVV Program Guidelines and Requirements . April 14, 2022 . Office of Health Insurance . New York State Department of Health
The 21st Century Cures Act, is a federal law, passed by Congress in December 2016, that in part requires all state Medicaid programs to implement an Electronic Visit Verification (EVV) system for personal care services (PCS) and home health care services (HHCS). All states must implement an EVV system to avoid a reduction in federal Medicaid ...
Revision 21-1; Effective Nov. 1, 2021 The Electronic Visit Verification (EVV) Policy Handbook provides EVV standards and policy requirements that program providers and Financial Management Services Agencies (FMSAs) contracted with Texas Health and Human Services Commission (HHSC) and managed care organizations (MCOs) must follow. The EVV Policy Handbook also includes requirements for Consumer ...
Geofence. DHS reduced the EVV geofence, which is a virtual perimeter around the home address of the member receiving services, from 500 miles to 500 feet from a member's home effective Dec. 1, 2023. Provider agencies using EVV systems must select the "community" option when providing services or visits outside the geofence range.
Electronic Visit Verification (EVV) NOTICE - Beginning December 16, 2022, certain Provider Type and Specialty Combinations will see a new question on the Additional Information page when completing a provider enrollment application. This information will also be displayed on the Provider Enrollment Summary.
Section 1903(l) of the Social Security Act, as added by section 12006 of the Cures Act (Pub. L. No. 114-255) and further amended by Public Law No. 115-222, stipulates that states will be subject to a reduction in Federal Medical Assistance Percentages (FMAP) if they do not implement Electronic Visit Verification (EVV) for personal care services by January 1, 2020, and for home healthcare ...
Electronic Visit Verification (EVV) is a computer-based system that verifies the occurrence of authorized personal attendant service visits by electronically documenting the precise time a service delivery visit begins and ends. Texas requires EVV for certain Medicaid funded home and community-based services provided through HHSC and MCOs.
Section 12006 (a) of the 21st Century Cures Act mandates that states implement Electronic Visit Verification (EVV) for all Medicaid-funded Personal Care Services (PCS) and Home Health Services (HHCS) that require an in-home visit by a provider. See the Manual Entries and Sandata Mobile Connect 2.0 bulletin posted Jan. 29, 2024.
Electronic Visit Verification Technical User Guide . April 2022 5 . 1 Electronic Visit Verification Overview . The . 21st Century Cures Act, is a federal law, passed by Congress in December 2016, that in part requires all state Medicaid programs to implement an Electronic Visit Verification (EVV)
These regulations apply to Medicaid-funded personal and health care services delivered at home and in community-based settings. For Medicaid billing in most states, the following must be captured in order for home care agencies to receive compensation for the visit being completed: Individual Receiving the Service; Date of Service
What is Electronic Visit Verification? The CURES Act was designed to improve the quality of care provided to individuals, enhance quality control, ... Providers who fail to comply with all state and federal EVV regulations are subject to having administrative sanctions listed in 13 CSR 70-3.030(4) imposed by the Missouri Medicaid Audit ...
The public comment period for proposed changes to regulations requiring electronic visit verification for the delivery of personal care services is open until November 23, 2020. Questions about the proposed regulations that are received by November 13 will be included in a Frequently Asked Questions document that will be made available through ...
Following a series of engagements with a wide variety of stakeholders, and after carefully considering input from Medicaid beneficiaries, family caregivers, providers, advocates, partner agencies, and solution providers, including information gathered from a Request for Information (RFI), in 2020 New York elected to proceed with the Choice Model for implementing Electronic Visit Verification ...
The third option to capture visits is through Fixed Visit Verification (FVV). This option should be used when the download of a mobile app or telephony is not available. Provider agencies using the Medicaid's EVV solution may purchase or lease an FVV device through Sandata. Providers can purchase FVV devices for a one-time cost of $85 per ...
Date. Training. Time. April 25, 2024. EVV Aggregator Training. 1:00 - 2:00 PM. There will be no additional trainings scheduled for EVV after April 25, 2024. Providers can still request an Ad Hoc EVV Training by emailing [email protected] to schedule a training. Getting Started.
Following enactment of P.L. 2023, ch. 576 (LD 2055), An Act to Prohibit the Department of Health and Human Services from Implementing Electronic Visit Verification for Hospice Providers Within the MaineCare Program Unless Mandated by the Federal Government, the Department is delaying the implementation of EVV requirements for hospice services ...