- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- COVID-19 Vaccines
- Occupational Therapy
- Healthy Aging
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board

The Heart's Electrical System: Anatomy and Function
Five components of electrical conduction make the heart beat
The electrical system of the heart is critical to how it functions . It controls the electrical impulses that cause your heart to beat and their conduction, which organizes the beating of your heart.
The movement of electrical signals across the heart is what is traced on an electrocardiogram (EKG). The EKG is also what allows irregularities in the heart's electrical system, and with them any related symptoms and medical conditions, to be assessed.
This article explains five components of the cardiac conduction system and how they work. It also discusses how heart disease or a heart attack can cause serious disruptions in the system.
Where Do Electrical Impulses Start in the Heart?
The heart generates its own electrical signal. This electrical signal is produced by a tiny structure known as the sinus node, located in the upper portion of the right atrium. The right atrium is one of four heart chambers and related valves , which include two atria at the top of the heart with two ventricles at the bottom.
The cardiac electrical signal controls the heartbeat in two ways. First, since each electrical impulse generates one heartbeat, the number of electrical impulses determines the heart rate . In a normal sinus rhythm, that rate will be between 60 and 100 beats per minute.
The sinus node signal also controls electrical conduction as it "spreads" across the heart. It causes the cells of the heart muscle to contract in the correct sequence, and ensures regular, efficient, and coordinated heartbeats. For this reason, the sinus node is often referred to as the heart's "natural pacemaker."
Components of the Cardiac Conduction System
Illustration by Mira Norian for Verywell Health
The components of the heart's electrical system, including the sinus node (SN) and atrioventricular node (AV node), are illustrated here. You can see the two atria and the two ventricles. Separating them is a layer of fibrous tissue, labeled the AV disc. This tissue keeps the electrical signal passing through the AV node.
In this figure:
- SN = sinus node
- AVN = AV node
- RA = right atrium
- LA = left atrium
- RV = right ventricle
- LV = left ventricle
- TV = tricuspid valve (the valve that separates the right atrium from the right ventricle)
- MV = mitral valve (the valve that separates the left atrium from the left ventricle)
The Heart's Electrical Signal Spreads Across the Atria
The electrical impulse originates in the sinus node. From there, it spreads across the right atrium and the left atrium (the top two chambers of the heart), causing both atria to contract. This is referred to as atrial depolarization, an action that pushes blood into the right and left ventricles, the bottom two chambers of the heart.
As the electrical impulse passes through the atria, it generates the so-called "P" wave on the EKG. The P wave is indicated by the solid red line on the EKG in the left side of the image above.
The Heart's Electrical Signal Reaches the AV Node
When the wave of electricity reaches the AV disc, it is stopped, except in the AV node. The impulse travels through the AV node at a slow, controlled rate toward the ventricles, so there is a pause in the electrical activity on the EKG, referred to as the PR interval. This is shown by the solid red line on the EKG in this figure.
This pause allows the atria to contract fully, emptying blood into the ventricles before the ventricles begin to contract.
The Heart's Electrical Signal Passes to the Ventricles
The specialized AV conduction system consists of the AV node (AVN), the "His bundle," and the right and left bundle branches (RBB and LBB). The AV node conducts the electrical impulse to the His bundle. The His bundle passes the signal to the right and left bundle branches.
The right and left bundle branches, in turn, send the electrical impulse to the right and left ventricles, respectively. The figure also shows that the LBB itself splits into the left anterior fascicle (LAF) and the left posterior fascicle (LPF).
The Heart's Electrical Signal Spreads Across the Ventricles
This figure shows the electrical impulse spreading throughout the right and left ventricles, causing these chambers to contract. As the electrical signal travels through the ventricles, it generates the “QRS complex” on the EKG. (The QRS complex is indicated by the solid red line on the EKG to the left.)
In this manner, the electrical system of the heart causes the heart muscle to contract and send blood to the organs of the body (via the left ventricle) and to the lungs (via the right ventricle).
Conduction Disorders and Treatments
AsiaVision / Getty Images
Heart block is a conduction disorder in which the heart's electrical signals are unable to move from the atria to the ventricles. This interference prevents the atria from telling the ventricles when to contract and pump blood.
In most cases of heart block, the electrical signals are weakened but do not stop completely. There are three degrees of heart block severity:
- First degree heart block: The least severe degree of heart block, in which the electrical signals are slowed but still reach your ventricles. Treatment may not be needed.
- Second degree heart block: In second degree AV block, some of the electrical impulses from the atria reach the ventricles, but some are blocked and never reach the ventricles. Depending on the underlying cause of this condition, a pacemaker may need to be considered.
- Third degree heart block: The most severe degree of heart block, in which electrical signals completely fail to reach the ventricles. If this happens, a person's pulse may dramatically slow, or there may be no pulse at all. A pacemaker is almost always required.
Another type of conduction disorder, bundle branch block , occurs when a blockage in the right or left bundle branch causes one ventricle to contract slightly slower than the other.
Bundle branch block by itself often does not require treatment. When it does, treatment involves managing the underlying health condition, be it heart disease, high blood pressure , a congenital (present at birth) heart defect, or something else.
Other Heart Electrical System Problems
- Sinus bradycardia ("brady" means slow) is the most common cause of a low heart rate and is caused by the SA node firing at a reduced rate.
- Sinus tachycardia ("tachy" means fast) refers to a rapid heart rate and can be caused by the SA node firing at an increased rate.
From the initiation of a heartbeat in the SA node through contraction of the ventricles, the cardiac electrical system causes the heart to contract in a coordinated manner, maximizing the efficiency of the beating heart.
Having a conduction disorder, in which the heart's electric pathway is disrupted, increases the risk of major complications, including cardiac arrest. Fortunately, there are ways to reduce your risk of a conduction disorder or related complications, including regular exercise and a heart-healthy diet.
American Heart Association. How the healthy heart works .
Mercy Health. Sinus tachycardia .
American Heart Association. What is an arrhythmia? .
Glover BM, Brugada P. Clinical handbook of cardiac electrophysiology . Springer.
Achilles JP, Withrow GW. The cardiac pump . In: Cardiovascular Physiology . 2013;2013(10):55-90. doi:10.1016/B978-0-323-08697-4.00004-6
Klabunde, RE. Cardiac cycle - atrial contraction (phase 1) . Cardiovascular Physiology Topics.
John Hopkins Medicine. Anatomy and Function of the Heart's Electrical System .
ACLS Medical Training. The Basics of ECG .
Johns Hopkins Medicine. Heart block .
American Heart Association. Heart conduction disorders .
American Heart Association. Bradycardia: Slow heart rate .
American Heart Association. Tachycardia: Slow heart rate .
National Heart, Lung, and Blood Institute. Conduction disorders .
Fogoros RN, Mandrola JM. Disorders of the heart rhythm: Basic principles. In: Fogoros’ Electrophysiologic Testing . Wiley Blackwell, 6th edition.
By Richard N. Fogoros, MD Richard N. Fogoros, MD, is a retired professor of medicine and board-certified in internal medicine, clinical cardiology, and clinical electrophysiology.
4 Steps of Cardiac Conduction
- Cell Biology
- Weather & Climate
- B.A., Biology, Emory University
- A.S., Nursing, Chattahoochee Technical College
Have you ever wondered what causes your heart to beat? Your heart beats as a result of the generation and conduction of electrical impulses. Cardiac conduction is the rate at which the heart conducts electrical impulses. These impulses cause the heart to contract and then relax. The constant cycle of heart muscle contraction followed by relaxation causes blood to be pumped throughout the body. Cardiac conduction can be influenced by various factors including exercise, temperature, and endocrine system hormones.
Step 1: Pacemaker Impulse Generation
The first step of cardiac conduction is impulse generation. The sinoatrial (SA) node (also referred to as the pacemaker of the heart) contracts, generating nerve impulses that travel throughout the heart wall . This causes both atria to contract. The SA node is located in the upper wall of the right atrium. It is composed of nodal tissue that has characteristics of both muscle and nervous tissue .
Step 2: AV Node Impulse Conduction
The atrioventricular (AV) node lies on the right side of the partition that divides the atria, near the bottom of the right atrium. When the impulses from the SA node reach the AV node, they are delayed for about a tenth of a second. This delay allows atria to contract and empty their contents into the ventricles prior to ventricle contraction.
Step 3: AV Bundle Impulse Conduction
The impulses are then sent down the atrioventricular bundle. This bundle of fibers branches off into two bundles and the impulses are carried down the center of the heart to the left and right ventricles .
Step 4: Purkinje Fibers Impulse Conduction
At the base of the heart, the atrioventricular bundles start to divide further into Purkinje fibers. When the impulses reach these fibers they trigger the muscle fibers in the ventricles to contract. The right ventricle sends blood to the lungs via the pulmonary artery . The left ventricle pumps blood to the aorta .
Cardiac Conduction and the Cardiac Cycle
Cardiac conduction is the driving force behind the cardiac cycle . This cycle is the sequence of events that occur when the heart beats. During the diastole phase of the cardiac cycle, the atria and ventricles are relaxed and blood flows into the atria and ventricles. In the systole phase, the ventricles contract sending blood to the rest of the body.
Cardiac Conduction System Disorders
Disorders of the heart's conduction system can cause problems with the heart's ability to function effectively. These problems are typically the result of a blockage that diminishes the rate of speed at which impulses are conducted. Should this blockage occur in one of the two atrioventricular bundle branches that lead to the ventricles, one ventricle may contract more slowly than the other. Individuals with bundle branch block typically don't experience any symptoms, but this issue can be detected with an electrocardiogram (ECG). A more serious condition, known as heart block, involves the impairment or blockage of electrical signal transmissions between the heart's atria and ventricles. Heart block electrical disorders range from first to third degree and are accompanied by symptoms ranging from light-headedness and dizziness to palpitations and irregular heartbeats.
Surkova, Elena, et al. " Left bundle branch block: from cardiac mechanics to clinical and diagnostic challenges ." EP Europace , vol. 19, no. 8, 2017, pp: 1251–1271, doi:10.1093/europace/eux061
Bazan, Victor, et al. " Contemporary Yield of 24-hour Holter Monitoring: Role of Inter-Atrial Block Recognition ." Journal of Atrial Fibrillation , vol. 12, no. 2, 2019, pp. 2225, doi: 10.4022/jafib.2225
- Heart Nodes and Electrical Conduction
- The Cardiac Cycle
- The Anatomy of the Heart, Its Structures, and Functions
- Atria of the Heart Function
- The Function of the Heart Ventricles
- The 3 Layers of the Heart Wall
- Anatomy of the Heart: Valves
- 10 Fascinating Facts About Your Heart
- Myocardium of the Heart
- Circulatory System: Pulmonary and Systemic Circuits
- How the Main Pulmonary Artery Delivers Blood to the Lungs
- Cardiovascular System
- Evolution of the Human Heart’s Four Chambers
- Artery Structure, Function, and Disease
- What Is Hemodynamics?
- Blood Composition and Function
- Anatomical Position
- Body Planes
- Terms of Movement
- Terms of Location
- Embryology Terms
- Classification
- Synovial Joint
- Joint Stability
- Skeletal Muscle
- Blood Vessels
- Head and Neck
- Cardiovascular System
- Respiratory System
- Urinary System
- Reproductive System
- Central Nervous System
- Cranial Fossae
- Pterygopalatine Fossa
- Infratemporal Fossa
- Mastoid Fossa
- Frontal Bone
- Sphenoid Bone
- Ethmoid Bone
- Temporal Bone
- Occipital Bone
- Nasal Skeleton
- Cranial Foramina
- Facial Expression
- Extraocular
- Mastication
- Sympathetic Innervation
- Parasympathetic Innervation
- Ophthalmic Nerve
- Maxillary Nerve
- Mandibular Nerve
- Nose and Sinuses
- Salivary Glands
- Oral Cavity
- Arterial Supply
- Venous Drainage
- Lacrimal Gland
- Basal Ganglia
- Pineal Gland
- Pituitary Gland
- Spinal Cord (Grey Matter)
- Medulla Oblongata
- Ascending Tracts
- Descending Tracts
- Visual Pathway
- Auditory Pathway
- Olfactory Nerve (CN I)
- Optic Nerve (CN II)
- Oculomotor Nerve (CN III)
- Trochlear Nerve (CN IV)
- Trigeminal Nerve (CN V)
- Abducens Nerve (CN VI)
- Facial Nerve (CN VII)
- Vestibulocochlear Nerve (CN VIII)
- Glossopharyngeal Nerve (CN IX)
- Vagus Nerve (CN X)
- Accessory Nerve (CN XI)
- Hypoglossal Nerve (CN XII)
- Dural Venous Sinuses
- Cavernous Sinus
- Anterior Triangle
- Posterior Triangle
- Cervical Spine
- Thyroid Gland
- Parathyroid Glands
- Suboccipital
- Suprahyoids
- Infrahyoids
- Phrenic Nerve
- Cervical Plexus
- Fascial Layers
- Tonsils (Waldeyer's Ring)
- Superior Mediastinum
- Anterior Mediastinum
- Middle Mediastinum
- Posterior Mediastinum
- Thoracic Spine
- Thoracic Cage
- Thymus Gland
- Mammary Glands
- Tracheobronchial Tree
- Superior Vena Cava
- Vertebral Column
- Superficial
- Intermediate
- Spinal Cord
- Quadrangular Space
- Triangular Interval
- Triangular Space
- Cubital Fossa
- Ulnar Tunnel
- Extensor Compartments
- Ulnar Canal
- Carpal Tunnel
- Anatomical Snuffbox
- Pectoral Region
- Shoulder Region
- Anterior Forearm
- Posterior Forearm
- Brachial Plexus
- Axillary Nerve
- Musculocutaneous Nerve
- Median Nerve
- Radial Nerve
- Ulnar Nerve
- Acromioclavicular Joint
- Sternoclavicular Joint
- Shoulder Joint
- Elbow Joint
- Radioulnar Joints
- Wrist Joint
- Metacarpophalangeal Joint
- Proximal Interphalangeal Joint
- Extensor Tendon Expansion
- Flexor Pulley System
- Femoral Triangle
- Femoral Canal
- Adductor Canal
- Popliteal Fossa
- Tarsal Tunnel
- Fascia Lata
- Gluteal Region
- Cutaneous Innervation
- Lumbar Plexus
- Sacral Plexus
- Femoral Nerve
- Obturator Nerve
- Sciatic Nerve
- Tibial Nerve
- Common Fibular Nerve
- Superficial Fibular Nerve
- Deep Fibular Nerve
- Tibiofibular Joints
- Ankle Joint
- Subtalar Joint
- Foot Arches
- Walking and Gaits
- Abdominal Cavity
- Calot’s Triangle
- The Peritoneum
- Inguinal Canal
- Hesselbach's Triangle
- Lumbar Spine
- Anterolateral Abdominal Wall
- Posterior Abdominal Wall
- Small Intestine
- Gallbladder
- Adrenal Glands
- Sciatic Foramina
- Pelvic Girdle
- Sacroiliac Joint
- Pelvic Floor
- Urinary Bladder
- Testes and Epididymis
- Spermatic Cord
- Prostate Gland
- Bulbourethral Glands
- Seminal Vesicles
- Fallopian (Uterine) Tubes
- Supporting Ligaments
- Pudendal Nerve
- Female Body
- Female Pelvis
- Male Pelvis
- Cardiovascular
- Gastrointestinal
- Respiratory
- Female Reproductive
- Male Reproductive
The Conducting System of the Heart
Original Author(s): Sophie White Last updated: April 24, 2023 Revisions: 31
- 1 Overview of Heart Conduction
- 2.1 Sinoatrial Node
- 2.2 Atrioventricular Node
- 2.3 Atrioventricular Bundle
- 2.4 Purkinje Fibres
- 3 Clinical Relevance: Artificial Pacemaker
The cardiac conduction system is a collection of nodes and specialised conduction cells that initiate and co-ordinate contraction of the heart muscle. It consists of:
- Sinoatrial node
- Atrioventricular node
- Atrioventricular bundle (bundle of His)
- Purkinje fibres
In this article, we shall look at the anatomy of the cardiac conduction system – its structure, function and clinical correlations.
Overview of Heart Conduction
The following sequence of electrical events occurs during one full contraction of the heart muscle:
- An excitation signal (an action potential) is created by the sinoatrial (SA) node .
- The wave of excitation spreads across the atria, causing them to contract.
- Upon reaching the atrioventricular (AV) node , the signal is delayed.
- It is then conducted into the bundle of His , down the interventricular septum.
- The bundle of His and the Purkinje fibres spread the wave impulses along the ventricles, causing them to contract.
We will now discuss the anatomy of the individual components involved in the conducting system.
Fig 1 – Animation of the spread of conduction through the heart
Components of the Cardiac Conduction System
Sinoatrial node.
The sinoatrial (SA) node is a collection of specialised cells (pacemaker cells), and is located in the upper wall of the right atrium, at the junction where the superior vena cava enters.
These pacemaker cells can spontaneously generate electrical impulses . The wave of excitation created by the SA node spreads via gap junctions across both atria, resulting in atrial contraction (atrial systole) – with blood moving from the atria into the ventricles.
The rate at which the SA node generates impulses is influenced by the autonomic nervous system:
- Sympathetic nervous system – increases firing rate of the SA node, and thus increases heart rate.
- Parasympathetic nervous system – decreases firing rate of the SA node, and thus decreases heart rate.
Atrioventricular Node
After the electrical impulses spread across the atria, they converge at the atrioventricular node – located within the atrioventricular septum, near the opening of the coronary sinus.
The AV node acts to delay the impulses by approximately 120ms , to ensure the atria have enough time to fully eject blood into the ventricles before ventricular systole.
The wave of excitation then passes from the atrioventricular node into the atrioventricular bundle.
Atrioventricular Bundle
The atrioventricular bundle (bundle of His) is a continuation of the specialised tissue of the AV node, and serves to transmit the electrical impulse from the AV node to the Purkinje fibres of the ventricles.
It descends down the membranous part of the interventricular septum, before dividing into two main bundles:
- Right bundle branch – conducts the impulse to the Purkinje fibres of the right ventricle
- Left bundle branch – conducts the impulse to the Purkinje fibres of the left ventricle.
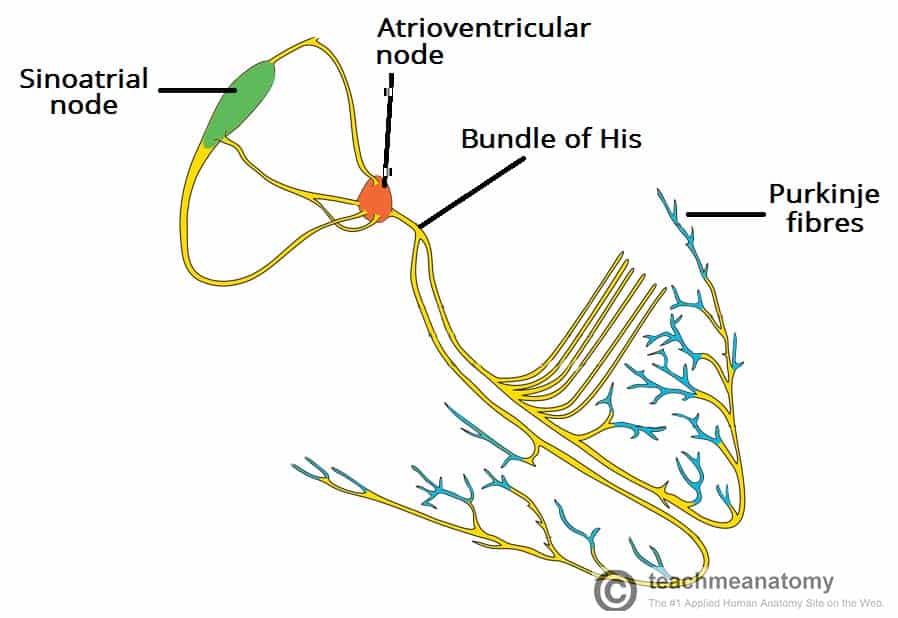
Fig 2 – Overview of the individual components of the heart conduction pathway
Purkinje Fibres
The Purkinje fibres (sub-endocardial plexus of conduction cells) are a network of specialised cells. They are abundant with glycogen and have extensive gap junctions.
These cells are located in the subendocardial surface of the ventricular walls, and are able to rapidly transmit cardiac action potentials from the atrioventricular bundle to the myocardium of the ventricles.
This rapid conduction allows coordinated ventricular contraction (ventricular systole) and blood is moved from the right and left ventricles to the pulmonary artery and aorta respectively.
Clinical Relevance: Artificial Pacemaker
An artificial pacemaker is a small electrical device commonly fitted to monitor and correct heart rate and rhythm. It is inserted into the chest under the left clavicle, with wires connected to the heart via the venous system.
The most common indication for a pacemaker is bradycardia . Once inserted, the pacemaker monitors the heart rate, and only fires if the rate becomes too slow. Pacemakers can also be used to treat some tachycardias, certain types of heart block and other rhythm abnormalities.
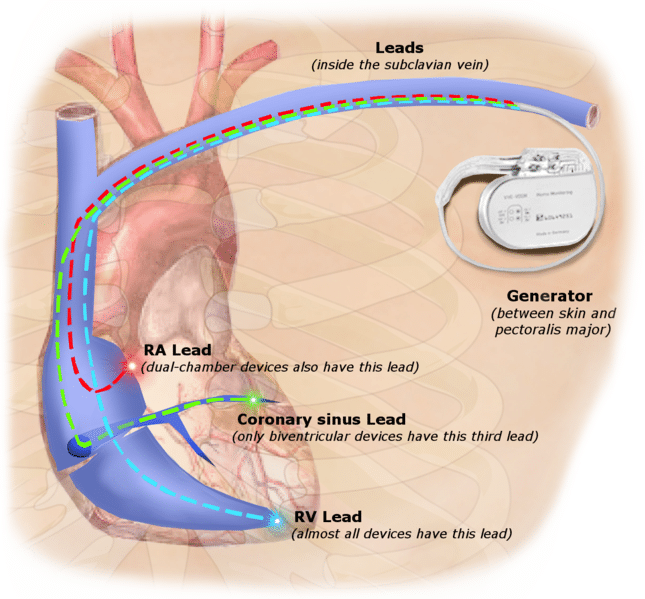
Fig 3 – There are various types of pacemakers; the most common are dual-chamber and single-chamber.
In this article, we shall look at the anatomy of the cardiac conduction system - its structure, function and clinical correlations.
These pacemaker cells can spontaneously generate electrical impulses . The wave of excitation created by the SA node spreads via gap junctions across both atria, resulting in atrial contraction (atrial systole) - with blood moving from the atria into the ventricles.
- Sympathetic nervous system - increases firing rate of the SA node, and thus increases heart rate.
- Parasympathetic nervous system - decreases firing rate of the SA node, and thus decreases heart rate.
After the electrical impulses spread across the atria, they converge at the atrioventricular node - located within the atrioventricular septum, near the opening of the coronary sinus.
- Right bundle branch - conducts the impulse to the Purkinje fibres of the right ventricle
- Left bundle branch - conducts the impulse to the Purkinje fibres of the left ventricle.
[start-clinical]
[end-clinical]
Found an error? Is our article missing some key information? Make the changes yourself here!
Once you've finished editing, click 'Submit for Review', and your changes will be reviewed by our team before publishing on the site.
We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy .
Privacy Overview
Heart Health
- Anatomy and Function of the Heart's Electrical System
The heart's electrical system
The heart is a pump made up of muscle tissue. Like all muscles, the heart needs a source of energy and oxygen to work. The heart's pumping action is controlled by an electrical system. This system organizes how the chambers of the heart contract and pump blood.
How does the heart beat?
Normally, as the electrical impulse moves through the heart, the heart contracts about 60 to 100 times a minute. The rate depends on a person's age.
Each contraction of the ventricles is 1 heartbeat. The atria contract a fraction of a second before the ventricles. The blood in the atria empties into the ventricles. Then the ventricles contract.
An electrical signal starts in the sinus node of the heart. This is also called the sinoatrial node (SA node). This is a small area of special cells in the right upper chamber (atrium) of the heart. The SA node creates an electrical signal 60 to 100 times per minute. The 2 upper chambers of the heart (atria) are stimulated first and contract for a short period of time before the 2 lower chambers of the heart (ventricles). The electrical signal spreads through the chambers of the heart. First, the atria are activated. The electrical signal then travels down through the conduction pathways to the heart's ventricles. This causes them to contract and pump out blood.
The electrical signal then travels from the sinus node to the atrioventricular node (AV node). There, the signals slow down for a very short period. Then they continue down the conduction pathway through a small group of cells called the bundle of His. The bundle of His divides into right and left pathways. These are called bundle branches. They stimulate the right and left ventricles. The signal travels into the ventricles. This completes 1 heartbeat.
Related Items
Diseases and conditions.
- Basic Anatomy of the Heart
- Wolff-Parkinson-White Syndrome
Pediatric Diseases and Conditions
Tests and procedures.
- Magnetic Resonance Imaging (MRI) of the Heart
- Have a Hearty Workout for Your Heart
- Making Changes to Prevent Heart Disease
- How Your Heart Works - Animation

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
10.4: Cardiac Cycle and Electrical Activity
- Last updated
- Save as PDF
- Page ID 105205

Cardiac Cycle Overview

The cardiac cycle refers to a single complete heartbeat, which includes one iteration of the lub and dub sounds heard through a stethoscope. During the cardiac cycle, the atria and ventricles work in a coordinated fashion so that blood is pumped efficiently through and out of the heart. The cardiac cycle includes two parts, called diastole and systole, which are illustrated in Figure \(\PageIndex{1}\).
- During diastole, the atria contract and pump blood into the ventricles, while the ventricles relax and fill with blood from the atria.
- During systole, the atria relax and collect blood from the lungs and body, while the ventricles contract and pump blood out of the heart.
Electrical Stimulation of the Heart

The normal, rhythmical beating of the heart is called sinus rhythm. It is established by the heart’s pacemaker cells, which are located in an area of the heart called the sinoatrial (SA) node (Figure \(\PageIndex{2}\)). The pacemaker cells create electrical signals by the movement of electrolytes (sodium, potassium, and calcium ions) into and out of the cells. For each cardiac cycle, an electrical signal rapidly travels first from the sinoatrial node to the right and left atria so they contract together. Then the signal travels to another node, called the atrioventricular (AV) node (also shown in Figure \(\PageIndex{2}\)), and from there to the right and left ventricles, which also contract together, just a split second after the atria contract.
The normal sinus rhythm of the heart is influenced by the autonomic nervous system through sympathetic and parasympathetic nerves. These nerves arise from two paired cardiovascular centers in the medulla of the brainstem. The parasympathetic nerves act to decrease the heart rate, and the sympathetic nerves act to increase the heart rate. Parasympathetic input normally predominates. Without it, the pacemaker cells of the heart would generate a resting heart rate of about 100 beats per minute, instead of a normal resting heart rate of about 72 beats per minute. The cardiovascular centers receive input from receptors throughout the body and act through the sympathetic nerves to increase the heart rate as needed. For example, increased physical activity is detected by receptors in muscles, joints, and tendons. These receptors send nerve impulses to the cardiovascular centers, causing sympathetic nerves to increase the heart rate. This allows more blood to flow to the muscles.
Besides the autonomic nervous system, other factors can also affect the heart rate. For example, thyroid hormones and adrenal hormones such as epinephrine can stimulate the heart to beat faster. The heart rate also increases when blood pressure drops or the body is dehydrated or overheated. On the other hand, cooling of the body and relaxation, among other factors, can contribute to a decrease in the heart rate.
Recall that cardiac muscle shares a few characteristics with both skeletal muscle and smooth muscle, but it has some unique properties of its own. Not the least of these exceptional properties is its ability to initiate an electrical potential at a fixed rate that spreads rapidly from cell to cell to trigger the contractile mechanism. This property is known as autorhythmicity . Neither smooth nor skeletal muscle can do this. Even though cardiac muscle has autorhythmicity, heart rate is modulated by the endocrine and nervous systems.
There are two major types of cardiac muscle cells: myocardial contractile cells and myocardial conducting cells. The myocardial contractile cells constitute the bulk (99 percent) of the cells in the atria and ventricles. Contractile cells conduct impulses and are responsible for contractions that pump blood through the body. The myocardial conducting cells (1 percent of the cells) form the conduction system of the heart. Except for Purkinje cells, they are generally much smaller than the contractile cells and have few of the myofibrils or filaments needed for contraction. Their function is similar in many respects to neurons, although they are specialized muscle cells. Myocardial conduction cells initiate and propagate the action potential (the electrical impulse) that travels throughout the heart and triggers the contractions that propel the blood.
Structure of Cardiac Muscle
Compared to the giant cylinders of skeletal muscle, cardiac muscle cells, or cardiomyocytes, are considerably shorter with much smaller diameters. Cardiac muscle also demonstrates striations, the alternating pattern of dark A bands and light I bands attributed to the precise arrangement of the myofilaments and fibrils that are organized in sarcomeres along the length of the cell (Figure \(\PageIndex{3}\) a). These contractile elements are virtually identical to skeletal muscle. T (transverse) tubules penetrate from the surface plasma membrane, the sarcolemma, to the interior of the cell, allowing the electrical impulse to reach the interior. The T tubules are only found at the Z discs, whereas in skeletal muscle, they are found at the junction of the A and I bands. Therefore, there are one-half as many T tubules in cardiac muscle as in skeletal muscle. In addition, the sarcoplasmic reticulum stores few calcium ions, so most of the calcium ions must come from outside the cells. The result is a slower onset of contraction. Mitochondria are plentiful, providing energy for the contractions of the heart. Typically, cardiomyocytes have a single, central nucleus, but two or more nuclei may be found in some cells.
Cardiac muscle cells branch freely. A junction between two adjoining cells is marked by a critical structure called an intercalated disc , which helps support the synchronized contraction of the muscle (Figure \(\PageIndex{3}\) b ). The sarcolemmas from adjacent cells bind together at the intercalated discs. They consist of desmosomes, specialized linking proteoglycans, tight junctions, and large numbers of gap junctions that allow the passage of ions between the cells and help to synchronize the contraction (Figure 19.17 c ). Intercellular connective tissue also helps to bind the cells together. The importance of strongly binding these cells together is necessitated by the forces exerted by contraction.
Cardiac muscle undergoes aerobic respiration patterns, primarily metabolizing lipids and carbohydrates. Myoglobin, lipids, and glycogen are all stored within the cytoplasm. Cardiac muscle cells undergo twitch-type contractions with long refractory periods followed by brief relaxation periods. The relaxation is essential so the heart can fill with blood for the next cycle. The refractory period is very long to prevent the possibility of tetany, a condition in which muscle remains involuntarily contracted. In the heart, tetany is not compatible with life, since it would prevent the heart from pumping blood.
Everyday Connection
Repair and replacement.
Damaged cardiac muscle cells have extremely limited abilities to repair themselves or to replace dead cells via mitosis. Recent evidence indicates that at least some stem cells remain within the heart that continue to divide and at least potentially replace these dead cells. However, newly formed or repaired cells are rarely as functional as the original cells, and cardiac function is reduced. In the event of a heart attack or MI, dead cells are often replaced by patches of scar tissue. Autopsies performed on individuals who had successfully received heart transplants show some proliferation of original cells. If researchers can unlock the mechanism that generates new cells and restore full mitotic capabilities to heart muscle, the prognosis for heart attack survivors will be greatly enhanced. To date, myocardial cells produced within the patient ( in situ ) by cardiac stem cells seem to be nonfunctional, although those grown in Petri dishes ( in vitro ) do beat. Perhaps soon this mystery will be solved, and new advances in treatment will be commonplace.
Conduction System of the Heart
If embryonic heart cells are separated into a Petri dish and kept alive, each is capable of generating its own electrical impulse followed by contraction. When two independently beating embryonic cardiac muscle cells are placed together, the cell with the higher inherent rate sets the pace, and the impulse spreads from the faster to the slower cell to trigger a contraction. As more cells are joined together, the fastest cell continues to assume control of the rate. A fully developed adult heart maintains the capability of generating its own electrical impulse, triggered by the fastest cells, as part of the cardiac conduction system. The components of the cardiac conduction system include the sinoatrial node, the atrioventricular node, the atrioventricular bundle, the atrioventricular bundle branches, and the Purkinje cells (Figure \(\PageIndex{4}\)).
Sinoatrial (SA) Node
Normal cardiac rhythm is established by the sinoatrial (SA) node , a specialized clump of myocardial conducting cells located in the superior and posterior walls of the right atrium in close proximity to the orifice of the superior vena cava. The SA node has the highest inherent rate of depolarization and is known as the pacemaker of the heart. It initiates the sinus rhythm , or normal electrical pattern followed by contraction of the heart.
This impulse spreads from its initiation in the SA node throughout the atria through specialized internodal pathways , to the atrial myocardial contractile cells and the atrioventricular node. The internodal pathways consist of three bands (anterior, middle, and posterior) that lead directly from the SA node to the next node in the conduction system, the atrioventricular node (see Figure \(\PageIndex{4}\)). The impulse takes approximately 50 ms (milliseconds) to travel between these two nodes. As the impulse reaches the atrioventricular septum, the connective tissue of the cardiac skeleton prevents the impulse from spreading into the myocardial cells in the ventricles except at the atrioventricular node. Figure \(\PageIndex{5}\) illustrates the initiation of the impulse in the SA node that then spreads the impulse throughout the atria to the atrioventricular node.
The electrical event, the wave of depolarization, is the trigger for muscular contraction. The wave of depolarization begins in the right atrium, and the impulse spreads across the superior portions of both atria and then down through the contractile cells. The contractile cells then begin contraction from the superior to the inferior portions of the atria, efficiently pumping blood into the ventricles.
Atrioventricular (AV) Node
The atrioventricular (AV) node is a second clump of specialized myocardial conductive cells, located in the inferior portion of the right atrium within the atrioventricular septum. The septum prevents the impulse from spreading directly to the ventricles without passing through the AV node. There is a critical pause before the AV node depolarizes and transmits the impulse to the atrioventricular bundle (see Figure \(\PageIndex{5}\), step 3). This delay in transmission is partially attributable to the small diameter of the cells of the node, which slow the impulse. Also, conduction between nodal cells is less efficient than between conducting cells. These factors mean that it takes the impulse approximately 100 ms to pass through the node. This pause is critical to heart function, as it allows the atrial cardiomyocytes to complete their contraction that pumps blood into the ventricles before the impulse is transmitted to the cells of the ventricle itself. With extreme stimulation by the SA node, the AV node can transmit impulses maximally at 220 per minute. This establishes the typical maximum heart rate in a healthy young individual. Damaged hearts or those stimulated by drugs can contract at higher rates, but at these rates, the heart can no longer effectively pump blood.
Atrioventricular Bundle (Bundle of His), Bundle Branches, and Purkinje Fibers
Arising from the AV node, the atrioventricular bundle , or bundle of His , proceeds through the interventricular septum before dividing into two atrioventricular bundle branches , commonly called the left and right bundle branches. The left bundle branch has two fascicles. The left bundle branch supplies the left ventricle, and the right bundle branch the right ventricle. Since the left ventricle is much larger than the right, the left bundle branch is also considerably larger than the right. Portions of the right bundle branch are found in the moderator band and supply the right papillary muscles. Because of this connection, each papillary muscle receives the impulse at approximately the same time, so they begin to contract simultaneously just prior to the remainder of the myocardial contractile cells of the ventricles. This is believed to allow tension to develop on the chordae tendineae prior to right ventricular contraction. There is no corresponding moderator band on the left. Both bundle branches descend and reach the apex of the heart where they connect with the Purkinje fibers (see Figure \(\PageIndex{5}\), step 4). This passage takes approximately 25 ms.
The Purkinje fibers are additional myocardial conductive fibers that spread the impulse to the myocardial contractile cells in the ventricles. They extend throughout the myocardium from the apex of the heart toward the atrioventricular septum and the base of the heart. The Purkinje fibers have a fast inherent conduction rate, and the electrical impulse reaches all of the ventricular muscle cells in about 75 ms (see Figure \(\PageIndex{5}\), step 5). Since the electrical stimulus begins at the apex, the contraction also begins at the apex and travels toward the base of the heart, similar to squeezing a tube of toothpaste from the bottom. This allows the blood to be pumped out of the ventricles and into the aorta and pulmonary trunk. The total time elapsed from the initiation of the impulse in the SA node until depolarization of the ventricles is approximately 225 ms.
Comparative Rates of Conduction System Firing
Since the SA node is the pacemaker, it reaches threshold faster than any other component of the conduction system. It will initiate the impulses spreading to the other conducting cells. The SA node, without nervous or endocrine control, would initiate a heart impulse approximately 80–100 times per minute. Although each component of the conduction system is capable of generating its own impulse, the rate progressively slows as you proceed from the SA node to the Purkinje fibers. Without the SA node, the AV node would generate a heart rate of 40–60 beats per minute. If the AV node were blocked, the atrioventricular bundle would fire at a rate of approximately 30–40 impulses per minute. The bundle branches would have an inherent rate of 20–30 impulses per minute, and the Purkinje fibers would fire at 15–20 impulses per minute. While a few exceptionally trained aerobic athletes demonstrate resting heart rates in the range of 30–40 beats per minute (the lowest recorded figure is 28 beats per minute for Miguel Indurain, a cyclist), for most individuals, rates lower than 50 beats per minute would indicate a condition called bradycardia. Depending upon the specific individual, as rates fall much below this level, the heart would be unable to maintain adequate flow of blood to vital tissues, initially resulting in decreasing loss of function across the systems, unconsciousness, and ultimately death.
Electrocardiogram
By careful placement of surface electrodes on the body, it is possible to record the complex, compound electrical signal of the heart. This tracing of the electrical signal is the electrocardiogram (ECG) , also commonly abbreviated EKG (K coming kardiology, from the German term for cardiology). Careful analysis of the ECG reveals a detailed picture of both normal and abnormal heart function, and is an indispensable clinical diagnostic tool.
A normal ECG tracing is presented in Figure \(\PageIndex{6}\). Each component, segment, and interval is labeled and corresponds to important electrical events, demonstrating the relationship between these events and contraction in the heart.
There are five prominent points on the ECG: the P wave, the QRS complex, and the T wave. The small P wave represents the depolarization of the atria. The atria begin contracting approximately 25 ms after the start of the P wave. The large QRS complex represents the depolarization of the ventricles, which requires a much stronger electrical signal because of the larger size of the ventricular cardiac muscle. The ventricles begin to contract as the QRS reaches the peak of the R wave. Lastly, the T wave represents the repolarization of the ventricles. The repolarization of the atria occurs during the QRS complex, which masks it on an ECG.The major segments and intervals of an ECG tracing are indicated in Figure \(\PageIndex{6}\). Segments are defined as the regions between two waves. Intervals include one segment plus one or more waves. For example, the PR segment begins at the end of the P wave and ends at the beginning of the QRS complex. The PR interval starts at the beginning of the P wave and ends with the beginning of the QRS complex. The PR interval is more clinically relevant, as it measures the duration from the beginning of atrial depolarization (the P wave) to the initiation of the QRS complex. Since the Q wave may be difficult to view in some tracings, the measurement is often extended to the R that is more easily visible. Should there be a delay in passage of the impulse from the SA node to the AV node, it would be visible in the PR interval. Figure \(\PageIndex{7}\) correlates events of heart contraction to the corresponding segments and intervals of an ECG.
ECG Abnormalities
Occassionally, an area of the heart other than the SA node will initiate an impulse that will be followed by a premature contraction. Such an area, which may actually be a component of the conduction system or some other contractile cells, is known as an ectopic focus or ectopic pacemaker. An ectopic focus may be stimulated by localized ischemia; exposure to certain drugs, including caffeine, digitalis, or acetylcholine; elevated stimulation by both sympathetic or parasympathetic divisions of the autonomic nervous system; or a number of disease or pathological conditions. Occasional occurences are generally transitory and nonlife threatening, but if the condition becomes chronic, it may lead to either an arrhythmia, a deviation from the normal pattern of impulse conduction and contraction, or to fibrillation, an uncoordinated beating of the heart.
While interpretation of an ECG is possible and extremely valuable after some training, a full understanding of the complexities and intricacies generally requires several years of experience. In general, the size of the electrical variations, the duration of the events, and detailed vector analysis provide the most comprehensive picture of cardiac function. For example, an amplified P wave may indicate enlargement of the atria, an enlarged Q wave may indicate a MI, and an enlarged suppressed or inverted Q wave often indicates enlarged ventricles. T waves often appear flatter when insufficient oxygen is being delivered to the myocardium. An elevation of the ST segment above baseline is often seen in patients with an acute MI, and may appear depressed below the baseline when hypoxia is occurring.
As useful as analyzing these electrical recordings may be, there are limitations. For example, not all areas suffering a MI may be obvious on the ECG. Additionally, it will not reveal the effectiveness of the pumping, which requires further testing, such as an ultrasound test called an echocardiogram or nuclear medicine imaging. It is also possible for there to be pulseless electrical activity, which will show up on an ECG tracing, although there is no corresponding pumping action. Common abnormalities that may be detected by the ECGs are shown in Figure \(\PageIndex{9}\).
External Automated Defibrillators
In the event that the electrical activity of the heart is severely disrupted, cessation of electrical activity or fibrillation may occur. In fibrillation, the heart beats in a wild, uncontrolled manner, which prevents it from being able to pump effectively. Atrial fibrillation (see Figure \(\PageIndex{9}\) b ) is a serious condition, but as long as the ventricles continue to pump blood, the patient’s life may not be in immediate danger. Ventricular fibrillation (see Figure \(\PageIndex{9}\) d ) is a medical emergency that requires life support, because the ventricles are not effectively pumping blood. In a hospital setting, it is often described as “code blue.” If untreated for as little as a few minutes, ventricular fibrillation may lead to brain death. The most common treatment is defibrillation, which uses special paddles to apply a charge to the heart from an external electrical source in an attempt to establish a normal sinus rhythm (Figure \(\PageIndex{10}\)). A defibrillator effectively stops the heart so that the SA node can trigger a normal conduction cycle. Because of their effectiveness in reestablishing a normal sinus rhythm, external automated defibrillators (EADs) are being placed in areas frequented by large numbers of people, such as schools, restaurants, and airports. These devices contain simple and direct verbal instructions that can be followed by nonmedical personnel in an attempt to save a life.
Coronavirus (COVID-19): Latest Updates | Visitation Policies Visitation Policies Visitation Policies Visitation Policies Visitation Policies | COVID-19 Testing | Vaccine Information Vaccine Information Vaccine Information
Health Encyclopedia
Anatomy and function of the electrical system, the heart's electrical system.
In the simplest of terms, the heart is a pump made up of muscle tissue. The heart's pumping action is controlled by an electrical conduction system that coordinates the contraction of the heart chambers.
How does the heart beat?
An electrical stimulus is generated in a special part of the heart muscle called the sinus node. It's also called the sinoatrial node (SA node). The sinus node is a small mass of special tissue in the right upper chamber of the heart (right atrium). In an adult, the sinus node sends out a regular electrical pulse 60 to 100 times per minute. This electrical pulse travels down through the conduction pathways. It causes the heart's lower chambers (ventricles) to contract and pump out blood. The right and left atria are stimulated first. They contract to push blood from the atria into the ventricles. The ventricles then contract to push blood out into the blood vessels of the body.
The original electrical impulse travels from the sinus node across the cells of your heart's right and left atria. The signal travels to the AV node (atrioventricular node). This node is between the atria and the ventricles. In the AV node, the impulses are slowed down for a very short time. This allows the atria to contract a fraction of a second before the ventricles. The blood from the atria empties into the ventricles before the ventricles contract. After passing through the AV node, the electrical current then goes down the conduction pathway. It goes through a pathway called the bundle of His, and into the ventricles. The bundle of His divides into right and left pathways (bundle branches) to give electrical stimulation to the right and left ventricles.
Normally at rest, the heart contracts about 60 to 100 times a minute depending on your age. In general, your heart rate slows as you age.

What can go wrong with the heart's electrical system?
Under some abnormal conditions, certain heart tissue is capable of starting a heartbeat, or becoming the "pacemaker," just like the sinus node. An abnormal heartbeat (arrhythmia) may occur when:
The heart's natural pacemaker (the sinus node) becomes diseased and slows down
The normal conduction pathway is interrupted
Another part of the heart takes over as pacemaker. This causes a faster or slower heartbeat.
Symptoms of an arrhythmia can include a feeling that your heart is fluttering (heart palpitations), shortness of breath, dizziness, or fainting.
You may need an ECG (electrocardiogram) to assess the rhythm of the heart. This painless test records the electrical activity of your heart with several small stickers attached to your chest. If the electrical rhythm is abnormal, you may need to be prescribed medicine. Or you may need a procedure to further investigate the cause or correct the rhythm.
Medical Reviewers:
- Callie Tayrien RN MSN
- Stacey Wojcik MBA BSN RN
- Steven Kang MD
- Ask a Medical Librarian Make an Appointment Physicians & Services Physicians who treat the Heart
The sinoatrial (sinus) node (1) initiates an electrical impulse that flows through the right and left atria (2), making them contract. When the electrical impulse reaches the atrioventricular node (3), it is delayed slightly. The impulse then travels down the bundle of His (4), which divides into the right bundle branch for the right ventricle (5) and the left bundle branch for the left ventricle (5). The impulse then spreads through the ventricles, making them contract.
- Overview of Arrhythmias
- Bundle Branch Block and Fascicular Block
- Second Opinion
Anatomy and Function of the Heart's Electrical System

The heart's electrical system
The heart is a pump made up of muscle tissue. Like all muscle, the heart needs a source of energy and oxygen to work. The heart's pumping action is controlled by an electrical system. This system that organizes how the chambers of the heart contract and pump blood.
How does the heart beat?
Normally, as the electrical impulse moves through the heart, the heart contracts about 60 to 100 times a minute. The rate depends on a person's age.
Each contraction of the ventricles is 1 heartbeat. The atria contract a fraction of a second before the ventricles. The blood in the atria empties into the ventricles. Then the ventricles contract.
An electrical signal starts in the sinus node of the heart. This is also called the sinoatrial node (SA node). This is a small area of special cells in the right upper chamber (atrium) of the heart. The sinus node creates an electrical signal 60 to 100 times per minute. The 2 upper chambers of the heart (atria) are stimulated first and contract for a short period of time before the 2 lower chambers of the heart (ventricles). The electrical signal spreads through the chambers of the heart. First, the atria are activated. The electrical signal then travels down through the conduction pathways to the heart's ventricles. This causes them to contract and pump out blood.
The electrical signal then travels from the sinus node to the atrioventricular node (AV node). There, the signals slow down for a very short period. Then they continue down the conduction pathway through a small group of cells called the bundle of His. The bundle of His divides into right and left pathways. These are called bundle branches. They stimulate the right and left ventricles. The signal travels into the ventricles. This completes 1 heartbeat.
- Pediatric Cardiology
- Our Services
- Chiari Malformation Center at Stanford Medicine Children's Health
Related Topics
Have a Hearty Workout for Your Heart
Making Changes to Prevent Heart Disease
Connect with us:
Download our App:
- Leadership Team
- Vision, Mission & Values
- The Stanford Advantage
- Government and Community Relations
- Get Involved
- Volunteer Services
- Auxiliaries & Affiliates
© 123 Stanford Medicine Children’s Health

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
17.3: Cardiac Muscle and Electrical Activity
- Last updated
- Save as PDF
- Page ID 22376
- Whitney Menefee, Julie Jenks, Chiara Mazzasette, & Kim-Leiloni Nguyen
- Reedley College, Butte College, Pasadena City College, & Mt. San Antonio College via ASCCC Open Educational Resources Initiative
By the end of this section, you will be able to:
- Describe the structure of cardiac muscle tissue and cells
- Identify and describe the components of the conducting system that distributes electrical impulses through the heart
Recall that cardiac muscle shares a few characteristics with both skeletal muscle and smooth muscle, but it has some unique properties of its own. Not the least of these exceptional properties is its ability to initiate an electrical potential at a fixed rate that spreads rapidly from cell to cell to trigger the contractile mechanism. This property is known as autorhythmicity . Skeletal muscle can not do this. Even though cardiac muscle has autorhythmicity, heart rate is modulated by the endocrine and nervous systems.
Structure of Cardiac Muscle Tissue and Cells
Compared to the giant cylinders of skeletal muscle, cardiac muscle cells, or cardiomyocytes, are considerably shorter with much smaller diameters. Cardiac muscle also demonstrates striations, the alternating pattern of dark A bands and light I bands attributed to the precise arrangement of the myofilaments and fibrils that are organized in sarcomeres along the length of the cell (Figure \(\PageIndex{1}\).a). These contractile elements are virtually identical to skeletal muscle. T (transverse) tubules penetrate from the surface plasma membrane, the sarcolemma, to the interior of the cell, allowing the electrical impulse to reach the interior. The T tubules are only found at the Z discs, whereas in skeletal muscle, they are found at the junction of the A and I bands. Therefore, there are one-half as many T tubules in cardiac muscle as in skeletal muscle. In addition, the sarcoplasmic reticulum of cardiomyocytes stores few calcium ions, so most of the calcium ions must come from outside the cells. The result is a slower onset of contraction. Mitochondria are plentiful, providing energy for the cross-bridge cycling responsible for contractions of the heart. Typically, cardiomyocytes have a single, central nucleus, but two or more nuclei may be found in some cells. Cardiac muscle undergoes aerobic respiration patterns, primarily metabolizing lipids and carbohydrates. Myoglobin, lipids, and glycogen are all stored within the cytoplasm.
Cardiac muscle cells branch freely. A junction between two adjoining cells is marked by a critical structure called an intercalated disc , which helps support the synchronized contraction of the muscle and structurally links the cells together (Figure \(\PageIndex{1}\)). Intercalated discs are formed by regions of sarcolemma with specialized integral membrane proteins. These form desmosomes, fasciae adherens, and large numbers of gap junctions. Desmosomes and fasciae adherens anchor the cells together. Fasciae adherens also anchor actin filaments of the sarcomere directly to the sarcolemma. Gap junctions allow the passage of ions from cell-to-cell through their sarcoplasm, a feature essential to producing synchronized contractions (Figure \(\PageIndex{1}\).c). Intercellular connective tissue also helps to bind the cells together. The importance of strongly binding these cells together is necessitated by the forces exerted by contraction; unlike skeletal muscle in which cells are the length of the organ to pull collectively on a bone via collagenous connective tissue attachments, smaller cardiac muscle cells pull on each other and ultimately on the dense connective tissue of the cardiac skeleton when they contract.

There are two major types of cardiac muscle cells: myocardial contractile cells and myocardial conducting cells. The myocardial contractile cells constitute the bulk (99 percent) of the cells in the myocardium of the atria and ventricles. Myocardial contractile cells are autorhythmic, but they are primarily responsible for the strong, synchronized contractions necessary to pump blood through the body. The myocardial conducting cells (1 percent of the cells) are generally much smaller than the contractile cells and have fewer myofibrils for contraction. Myocardial conducting cells are specialized to initiate and propagate the electrical activity that travels throughout the heart and triggers the contractions of the myocardial contractile cells that propel the blood. If embryonic heart cells are separated into a Petri dish and kept alive, each is capable of generating its own electrical impulse (also referred to as a wave of depolarization or an action potential) that is followed by contraction (the capability that is described as autorhythmicity). When two independently beating embryonic cardiac muscle cells are placed together, the cell with the faster inherent rate sets the pace, and the impulse spreads from the faster to the slower cell to trigger a contraction in such rapid succession that they appear to contract in unison. As more cells are joined together, the fastest cell continues to assume control of the rate. A fully developed adult heart maintains the capability to generate its own electrical activity, triggered by the fastest cells. The fastest cells are the myocardial conducting cells. The slower cells (which are also stronger) are the myocardial contractile cells.
EVERYDAY CONNECTION
Repair and Replacement of Cardiac Muscle
Damaged cardiac muscle cells have extremely limited abilities to repair themselves or to replace dead cells via mitosis. Recent evidence indicates that at least some stem cells remain within the heart that continue to divide and at least potentially replace these dead cells. However, newly formed or repaired cells are rarely as functional as the original cells, and cardiac function is reduced. In the event of a heart attack or myocardial infarction (MI), dead cells are often replaced by patches of scar tissue in a process called fibrosis. Autopsies performed on individuals who had successfully received heart transplants show some proliferation of original cells. If researchers can unlock the mechanism that generates new cells and restore full mitotic capabilities to heart muscle, the prognosis for heart attack survivors will be greatly enhanced. To date, myocardial cells produced within the patient ( in situ ) by cardiac stem cells seem to be nonfunctional, although those grown in Petri dishes ( in vitro ) do beat. Perhaps soon this mystery will be solved, and new advances in treatment will be commonplace.
Conducting System of the Heart
The myocardial conducting cells are concentrated in specific areas of the heart that make up the Conducting System. The components of the cardiac conducting system include the sinoatrial node, the atrioventricular node, the atrioventricular bundle, the atrioventricular bundle branches, and the Purkinje fibers (Figure \(\PageIndex{2}\)).

Sinoatrial (SA) Node
Normal cardiac rhythm is established by the sinoatrial (SA) node , a specialized clump of myocardial conducting cells located in the posterosuperior walls of the right atrium in close proximity to the orifice of the superior vena cava. The myocardial conducting cells of the SA node have the highest inherent rate of electrical signal initiation, so the SA node is known as the pacemaker of the heart. It initiates the sinus rhythm , or normal electrical pattern followed by contraction of the heart.
This impulse spreads from its initiation in the SA node throughout the atria through specialized internodal pathways , to the atrial myocardial contractile cells and the atrioventricular node. The internodal pathways consist of three bands (anterior, middle, and posterior) of myocardial conducting cells that lead directly from the SA node to the next node in the conducting system, the atrioventricular node (see Figure \(\PageIndex{2}\)). The impulse takes approximately 50 ms (milliseconds, thousandths of a second) to travel between these two nodes. The relative importance of this pathway has been debated since the impulse would reach the atrioventricular node simply following the cell-by-cell pathway through the contractile cells of the myocardium in the atria. In addition, there is a specialized pathway called Bachmann’s bundle or the interatrial band that conducts the impulse directly from the right atrium to the left atrium. Regardless of the pathway, as the impulse reaches the atrioventricular septum, the insulating connective tissue of the cardiac skeleton prevents the impulse from spreading into the myocardial cells in the ventricles except at the atrioventricular node. Figure \(\PageIndex{3}\) illustrates the initiation of the impulse in the SA node that then spreads the impulse throughout the atria to the atrioventricular node.

The electrical event (the wave of electrical signal) spreads the signal through the conducting system, but it is also the trigger for muscular contraction of the atria. The wave of electrical signal begins in the right atrium, and the impulse spreads across the superior portions of both atria and then down through the contractile cells. The contractile cells then begin contraction from the superior to the inferior portions of the atria, efficiently pumping blood into the ventricles.
Atrioventricular (AV) Node
The atrioventricular (AV) node is a second clump of specialized myocardial conducting cells, located in the inferior portion of the right atrium within the atrioventricular septum. The septum contains the dense irregular connective tissue of the cardiac skeleton that prevents the impulse from spreading directly to the ventricles without passing through the AV node. There is a critical pause before the AV node activates and transmits the electrical impulse to the atrioventricular bundle (see Figure \(\PageIndex{3}\), step 3). This delay in transmission is partially attributable to the small diameter of the cells of the node, which slow the impulse. Also, conduction between nodal cells is less efficient than between conducting cells. These factors mean that it takes the impulse approximately 100 ms to pass through the node. This pause is critical to heart function, as it allows the atrial cardiomyocytes to complete their contraction that pumps blood into the ventricles before the impulse is transmitted to the cells of the ventricle itself. With extreme stimulation by the SA node, the AV node can transmit impulses maximally at 220 per minute. This establishes the typical maximum heart rate in a healthy young individual. Damaged hearts or those stimulated by drugs can contract at higher rates, but at these rates, the heart can no longer effectively pump blood.
Atrioventricular Bundle (Bundle of His), Bundle Branches, and Subendocardial Conducting Network (Purkinje Fibers)
Arising from the AV node, the atrioventricular bundle , or bundle of His , proceeds into the interventricular septum before dividing into two atrioventricular bundle branches , commonly called the left and right bundle branches. The left bundle branch supplies the left ventricle, and the right bundle branch the right ventricle. Since the left ventricle is much larger than the right, the left bundle branch is also considerably larger than the right. Portions of the right bundle branch are found in the moderator band and supply the right papillary muscles. Because of this connection, each papillary muscle receives the impulse at approximately the same time, so they begin to contract simultaneously just prior to the remainder of the myocardial contractile cells of the ventricles. This is believed to allow tension to develop on the chordae tendineae prior to right ventricular contraction. There is no corresponding moderator band on the left. Both bundle branches descend and reach the apex of the heart where they connect with the subendocardial conducting network, or Purkinje fibers (see Figure \(\PageIndex{3}\), step 4). This passage takes approximately 25 ms.
The subendocardial conducting network , or Purkinje fibers, are additional myocardial conducting fibers that spread the impulse to the myocardial contractile cells in the ventricles. They extend throughout the myocardium from the apex of the heart toward the atrioventricular septum and the base of the heart at the top of the ventricles. The subendocardial conducting network has a fast inherent conduction rate, and the electrical impulse reaches all of the ventricular muscle cells in about 75 ms (see Figure \(\PageIndex{3}\), step 5). Since the electrical stimulus begins at the apex, the contraction also begins at the apex and travels toward the base of the heart, similar to squeezing a tube of toothpaste from the bottom. This allows the blood to be pumped out of the ventricles and into the aorta and pulmonary trunk. The total time elapsed from the initiation of the impulse in the SA node until initiation of impulse in the ventricles is approximately 225 ms.
Electrocardiogram
By careful placement of surface electrodes on the body, it is possible to record the complex, compound electrical signal of the heart. This tracing of the electrical signal is the electrocardiogram (ECG) , also commonly abbreviated EKG (K coming from kardiology, the German spelling of cardiology). Careful analysis of the ECG reveals a detailed picture of both normal and abnormal heart function, and is an indispensable clinical diagnostic tool. The standard electrocardiograph (the instrument that generates an ECG) uses 3, 5, or 12 leads. The greater the number of leads an electrocardiograph uses, the more information the ECG provides. The term “lead” may be used to refer to the cable from the electrode to the electrical recorder, but it typically describes the voltage difference between two of the electrodes. The 12-lead electrocardiograph uses 10 electrodes placed in standard locations on the patient’s skin (Figure \(\PageIndex{4}\)). In continuous ambulatory electrocardiographs, the patient wears a small, portable, battery-operated device known as a Holter monitor, or simply a Holter, that continuously monitors heart electrical activity, typically for a period of 24 hours during the patient’s normal routine.

The ECG measures and graphs electrical activity over the time of each cardiac cycle that visually represents the spread of the electrical impulse through the conducting system (Figure \(\PageIndex{5}\)). The spread of electrical impulse from the SA node that initiates the cardiac cycle and causes atrial systole is visible in the P wave. The spread of electrical impulse from the AV node through the AV bundle and bundle branches is visible as the portion of the ECG with the largest amplitude (height), the QRS complex. The T wave (and a portion of the QRS complex) measure the electrical activity associated with repolarization, the physiological reset required to prepare for the next cardiac cycle.

ECG Abnormalities
Occasionally, an area of the heart other than the SA node will initiate an impulse that will be followed by a premature contraction. Such an area, which may actually be a component of the conducting system or some other contractile cells, is known as an ectopic focus or ectopic pacemaker. An ectopic focus may be stimulated by localized ischemia (reduced blood flow to an area, depriving it of nutrients); exposure to certain drugs, including caffeine, digitalis, or acetylcholine; elevated stimulation by both sympathetic or parasympathetic divisions of the autonomic nervous system; or a number of disease or pathological conditions. Occasional occurrences are generally transitory and nonlife-threatening, but if the condition becomes chronic, it may lead to either an arrhythmia, a deviation from the normal pattern of impulse conduction and contraction, or to fibrillation, an uncoordinated beating of the heart.
While interpretation of an ECG is possible and extremely valuable after some training, a full understanding of the complexities and intricacies generally requires several years of experience. In general, the size of the electrical variations, the duration of the events, and detailed vector analysis provide the most comprehensive picture of cardiac function. For example, an amplified P wave may indicate enlargement of the atria, an enlarged Q wave may indicate a myocardial infarction (MI, heart attack), and an enlarged suppressed or inverted Q wave often indicates enlarged ventricles. T waves often appear flatter when insufficient oxygen is being delivered to the myocardium. An elevation of the ST segment above baseline is often seen in patients with an acute MI, and may appear depressed below the baseline when hypoxia is occurring.
As useful as analyzing these electrical recordings may be, there are limitations. For example, not all areas suffering a MI may be obvious on the ECG. Additionally, it will not reveal the effectiveness of the pumping, which requires further testing, such as an ultrasound test called an echocardiogram or nuclear medicine imaging. It is also possible for there to be pulseless electrical activity, which will show up on an ECG tracing, although there is no corresponding pumping action. Common abnormalities that may be detected by the ECGs are shown in Figure \(\PageIndex{6}\).

Figure \(\PageIndex{6}\): Common ECG Abnormalities. (a) In a second-degree or partial block, one-half of the P waves are not followed by the QRS complex and T waves while the other half are. (b) In atrial fibrillation, the electrical pattern is abnormal prior to the QRS complex, and the frequency between the QRS complexes has increased. (c) In ventricular tachycardia, the shape of the QRS complex is abnormal. (d) In ventricular fibrillation, there is no normal electrical activity. (e) In a third-degree block, there is no correlation between atrial activity (the P wave) and ventricular activity (the QRS complex). (Image credit: "Cardiac Arrhythmias" by OpenStax is licensed under CC BY 3.0 )
Automated External Defibrillators (AEDs)
In the event that the electrical activity of the heart is severely disrupted, cessation of electrical activity or fibrillation may occur. In fibrillation, the heart beats in a wild, uncontrolled manner, which prevents it from being able to pump effectively. Atrial fibrillation (see Figure \(\PageIndex{6}\).b) is a serious condition, but as long as the ventricles continue to pump blood, the patient’s life may not be in immediate danger. Ventricular fibrillation (see Figure \(\PageIndex{6}\).d) is a medical emergency that requires life support, because the ventricles are not effectively pumping blood. In a hospital setting, it is often described as “code blue.” If untreated for as little as a few minutes, ventricular fibrillation may lead to brain death. The most common treatment is defibrillation, which uses special paddles to apply a charge to the heart from an external electrical source in an attempt to establish a normal sinus rhythm (Figure \(\PageIndex{7}\)). A defibrillator effectively stops the heart so that the SA node can trigger a normal conduction cycle. Because of their effectiveness in reestablishing a normal sinus rhythm, external automated defibrillators (EADs) are being placed in areas frequented by large numbers of people, such as schools, restaurants, and airports. These devices contain simple and direct verbal instructions that can be followed by nonmedical personnel in an attempt to save a life.

Disorders of the Conducting System
A heart block refers to an interruption in the normal conduction pathway. The nomenclature for these is very straightforward. SA nodal blocks occur within the SA node. AV nodal blocks occur within the AV node. Infra-Hisian blocks involve the bundle of His. Bundle branch blocks occur within either the left or right atrioventricular bundle branches. Hemiblocks are partial and occur within one or more fascicles of the atrioventricular bundle branch. Clinically, the most common types are the AV nodal and infra-Hisian blocks.
AV blocks are often described by degrees. A first-degree or partial block indicates a delay in conduction between the SA and AV nodes. This can be recognized on the ECG as an abnormally long PR interval. A second-degree or incomplete block occurs when some impulses from the SA node reach the AV node and continue, while others do not. In this instance, the ECG would reveal some P waves not followed by a QRS complex, while others would appear normal. In the third-degree or complete block, there is no correlation between atrial activity (the P wave) and ventricular activity (the QRS complex). Even in the event of a total SA block, the AV node will assume the role of pacemaker and continue initiating contractions at 40–60 contractions per minute, which is adequate to maintain consciousness. Second- and third-degree blocks are demonstrated on the ECG presented in Figure \(\PageIndex{6}\).
When arrhythmias become a chronic problem, the heart maintains a junctional rhythm, which originates in the AV node. In order to speed up the heart rate and restore full sinus rhythm, a cardiologist can implant an artificial pacemaker , which delivers electrical impulses to the heart muscle to ensure that the heart continues to contract and pump blood effectively. These artificial pacemakers are programmable by the cardiologists and can either provide stimulation temporarily upon demand or on a continuous basis. Some devices also contain built-in defibrillators.
Heart Rates
Heart rates (HRs) vary considerably, not only with exercise and fitness levels, but also with age. Newborn resting HRs may be 120 bpm. Resting HR gradually decreases until young adulthood and then gradually increases again with age.
Maximum HRs are normally in the range of 200–220 bpm, although there are some extreme cases in which they may reach higher levels. As one ages, the ability to generate maximum rates decreases. This may be estimated by taking the maximal value of 220 bpm and subtracting the individual’s age. So a 40-year-old individual would be expected to hit a maximum rate of approximately 180 bpm, and a 60-year-old person would achieve 160 bpm.
Heart rate is adjusted by chemical signals from the endocrine system as well as nervous signals that emerge from the medulla oblongata in the brainstem and travel to the heart via the vagus nerve (parasympathetic nervous system) to slow down the heart rate or via the sympathetic cardiac nerve (sympathetic nervous system) to speed up the heart rate. Both nerve pathways send branches to both the SA and AV nodes, and the sympathetic nervous system also sends neurons to portions of both the atria and ventricles. Without any nervous stimulation, the SA node would establish a sinus rhythm of approximately 100 bpm. Since resting rates are considerably less than this, it becomes evident that parasympathetic stimulation normally slows HR. Reducing the parasympathetic stimulation allows the heart rate to approach 100 bpm. Increasing the heart rate above 100 bpm involves sympathetic stimulation.
DISORDERS OF THE...
Heart: Abnormal Heart Rates
For an adult, normal resting HR will be in the range of 60–100 bpm. Bradycardia is the condition in which resting rate drops below 60 bpm, and tachycardia is the condition in which the resting rate is above 100 bpm. Trained athletes typically have very low HRs. If the patient is not exhibiting other symptoms, such as weakness, fatigue, dizziness, fainting, chest discomfort, palpitations, or respiratory distress, bradycardia is not considered clinically significant. However, if any of these symptoms are present, they may indicate that the heart is not providing sufficient oxygenated blood to the tissues. The term relative bradycardia may be used with a patient who has a HR in the normal range but is still suffering from these symptoms. Most patients remain asymptomatic as long as the HR remains above 50 bpm.
Bradycardia may be caused by either inherent factors or causes external to the heart. While the condition may be inherited, typically it is acquired in older individuals. Inherent causes include abnormalities in either the SA or AV node. If the condition is serious, a pacemaker may be required. Other causes include ischemia to the heart muscle or diseases of the heart vessels or valves. External causes include metabolic disorders, pathologies of the endocrine system often involving the thyroid, electrolyte imbalances, neurological disorders including inappropriate autonomic responses, autoimmune pathologies, over-prescription of beta blocker drugs that reduce HR, recreational drug use, or even prolonged bed rest. Treatment relies upon establishing the underlying cause of the disorder and may necessitate supplemental oxygen.
Tachycardia is not normal in a resting patient but may be detected in pregnant women or individuals experiencing extreme stress. In the latter case, it would likely be triggered by stimulation from the limbic system or disorders of the autonomic nervous system. In some cases, tachycardia may involve only the atria. Some individuals may remain asymptomatic, but when present, symptoms may include dizziness, shortness of breath, lightheadedness, rapid pulse, heart palpitations, chest pain, or fainting (syncope). While tachycardia is defined as a HR above 100 bpm, there is considerable variation among people. Further, the normal resting HRs of children are often above 100 bpm, but this is not considered to be tachycardia. Many causes of tachycardia may be benign, but the condition may also be correlated with fever, anemia, hypoxia, hyperthyroidism, hypersecretion of catecholamines, some cardiomyopathies, some disorders of the valves, and acute exposure to radiation. Elevated rates in an exercising or resting patient are normal and expected. Resting rate should always be taken after recovery from exercise. Treatment depends upon the underlying cause but may include medications, implantable cardioverter defibrillators, ablation, or surgery.
Concept Review
The heart is regulated by both neural and endocrine control, yet it initiates its own electrical impulse at an intrinsic rate followed by muscular contraction. The myocardial conducting cells within the heart establish the heart rate and transmit it through the myocardium. The myocardial contractile cells contract and propel the blood. The normal path of transmission for the conductive cells is the sinoatrial (SA) node, internodal pathways, atrioventricular (AV) node, atrioventricular (AV) bundle, bundle branches, and Purkinje fibers. Normal resting heart rate is in the range of 60 to 100 bpm.
Review Questions
Q. Which of the following distinguishes cardiac muscle cells from skeletal muscle cells?
A. Only cardiac muscle contains a sarcoplasmic reticulum.
B. Only cardiac muscle has striations.
C. Only cardiac muscle is capable of autorhythmicity.
D. Only cardiac muscle has a high concentration of mitochondria.
Q. Which component of the heart's conducting system would have the slowest rate of firing?
A. atrioventricular node
B. atrioventricular bundle
C. bundle branches
D. subendocardial conducting network
Critical Thinking Questions
Q. How does the delay of the impulse at the atrioventricular node contribute to cardiac function?
A. It ensures sufficient time for the atrial muscle to contract and pump blood into the ventricles prior to the impulse being conducted into the lower chambers.
Q. How do intercalated discs aid contraction of the heart?
A. Intercalated discs consist of desmosomes, fasciae adherens, and gap junctions. Desmosomes and fasciae adherens create strong connections between adjacent cardiac muscle cells that will contract against one another. Gap junctions within the intercalated discs allow impulses to spread from one cardiac muscle cell to another, allowing ions to flow between adjacent cells, propagating the electrical impulse to contract, and ensuring coordinated contractions.
Q. Why is it important that the conducting system initiates ventricular systole from the apex of the heart?
A. Initiation of ventricular systole at the apex of heart allows the blood to be squeezed from the bottom-up toward the semilunar valves into the ascending aorta and pulmonary trunk.
Contributors and Attributions
OpenStax Anatomy & Physiology (CC BY 4.0). Access for free at https://openstax.org/books/anatomy-and-physiology

- DNA Replication
- Active Transport
- Cellular Receptors
- Endocytosis and Exocytosis
- Enzyme Inhibition
- Enzyme Kinetics
- Protein Structure
- Transcription of DNA
- Translation of DNA
- Anaerobic Respiration
- Electron Transport Chain
- Gluconeogenesis
- Calcium Regulation
- External Balance of Potassium
- Internal Balance of Potassium
- Sodium Regulation
- Cell Membrane
- Endoplasmic Reticulum
- Golgi Apparatus
- Mitochondria
- Blood Vessels
- Cellular Adaptations
- Epithelial Cells
- Muscle Histology
- Structure of Glands
- Control of Stroke Volume
- Control of Heart Rate
- Cardiac Cycle
- Cardiac Pacemaker Cells
- Conduction System
- Contraction of Cardiac Muscle
- Ventricular Action Potentials
- Blood Flow in Vessels
- Control of Blood Pressure
- Capillary Exchange
- Flow In Peripheral Circulation
- Venous Return
- Cardiac Muscle
- Hepatic Circulation
- Skeletal Muscle
- Airway Resistance
- Lung Volumes
- Mechanics of Breathing
- Gas Exchange
- Oxygen Transport in The Blood
- Transport of Carbon Dioxide in the Blood
- Ventilation-Perfusion Matching
- Chemoreceptors
- Cough Reflex
- Neural Control of Ventilation
- Respiratory Regulation of Acid-Base Balance
- Responses of The Respiratory System to Stress
- Regulation of Saliva
- Secretion of Saliva
- Gastric Acid Production
- Gastric Mucus Production
- Digestion and Absorption
- Histology and Cellular Function of the Small Intestine
- Absorption in the Large Intestine
- Large Intestinal Motility
- Bilirubin Metabolism
- Carbohydrate Metabolism in the Liver
- Lipid Metabolism in the Liver
- Protein and Ammonia Metabolism in the Liver
- Storage Functions of the Liver
- Bile Production
- Function of The Spleen
- Exocrine Pancreas
- Somatostatin
- Proximal Convoluted Tubule
- Loop of Henle
- Distal Convoluted Tubule and Collecting Duct
- Storage Phase of Micturition
- Voiding Phase of Micturition
- Antidiuretic Hormone
- Renin-Angiotensin-Aldosterone System
- Urinary Regulation of Acid-Base Balance
- Water Filtration and Reabsorption
- Development of the Reproductive System
- Gametogenesis
- Gonadotropins and the Hypothalamic Pituitary Axis
- Menstrual Cycle
- Placental Development
- Fetal Circulation
- Maternal Adaptations in Pregnancy
- Cells of the Nervous System
- Central Nervous System
- Cerebrospinal Fluid
- Neurotransmitters
- Peripheral Nervous System
- Action Potential
- Excitatory and Inhibitory Synaptic Signalling
- Resting Membrane Potential
- Synaptic Plasticity
- Synaptic Transmission
- Ascending Tracts
- Auditory Pathway
- Consciousness and Sleep
- Modalities of Sensation
- Pain Pathways
- Sensory Acuity
- Visual Pathway
- Descending Tracts
- Lower Motor Neurones
- Muscle Stretch Reflex
- Upper Motor Neurones
- Aqueous Humour
- Ocular Accommodation
- Thyroid Gland
- Parathyroid Glands
- Adrenal Medulla
- Zona Glomerulosa
- Zona Fasciculata
- Zona Reticularis
- Endocrine Pancreas
- The Hypothalamus
- Anterior Pituitary
- Posterior Pituitary
- White Blood Cells – Summary
- Barriers to Infection
- Infection Recognition Molecules
- Phagocytosis
- The Complement System
- Antigen Processing and Presentation
- Primary and Secondary Immune Responses
- T Cell Memory
- Acute Inflammation
- Autoimmunity
- Chronic Inflammation
- Hypersensitivity Reactions
- Immunodeficiency
- Types of Immunity
- Antibiotics
- Viral Infection
- Blood Groups
- Coagulation
- Erythropoiesis
- Iron Metabolism
- Mononuclear Phagocyte System
Original Author(s): Meghna Ray Last updated: 19th December 2023 Revisions: 8
- 1 The ECG leads
- 2 Reading an ECG
- 3.1 Components of the ECG trace
- 4 Clinical Relevance – STEMI vs NSTEMI
The electrocardiogram (ECG) is used to trace the electrical activity in cardiac tissue. It looks at how electrical impulses travel through the heart from various angles. It is used clinically to identify and locate pathology within the cardiac conducting system and within cardiac muscle.
This article covers the physiology underpinning ECGs, as well as explaining pathological ECG traces and how they arise. Some common, clinically relevant, ECG traces will also be covered.
The ECG leads
ECGs are most commonly measured using either 3 leads or 12 leads . The term ‘lead’ is slightly confusing, in that 12 lead ECGs actually only have 10 physical electrodes . These electrodes, however, generate 12 different ‘views’ of the heart. These ‘views’ are called ‘leads’.
In a 12 lead ECG there are 6 chest electrodes (V1-V6) and 4 limb electrodes. These come together to give the 12 leads, or views, of the heart. This can be useful in visualising the electrical activity of the heart from different views, and therefore to localise pathology.
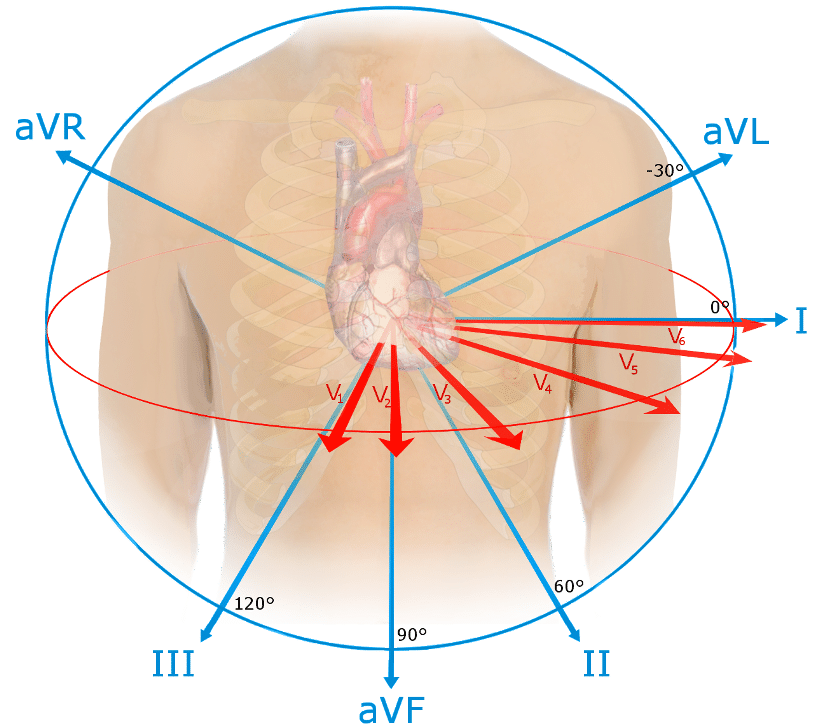
Figure 1 – The 12 ‘views’ of the heart in a 12 lead ECG
The leads can also be grouped together to give ‘territories’ of the heart. These correspond to the area of the heart that they are measuring the electrical activity from and also the coronary arteries which supply it. This can be useful clinically, especially in the case of a STEMI, as is outlined later.
Reading an ECG
ECG tracings are recorded on a specific type of paper, as shown in the example below. There are certain measurements to be aware of here:
- Small square = 0.04 secs
- Large square (5 small squares) = 0.2 secs
- 5 large squares = 1 second
- 300 large squares = 1 minute
Fig 2 – The specifics of ECG recording paper
Remembering these measurements is essential in reading an ECG trace, as it allows you to calculate the rate, and also assess whether there are any abnormalities in the length of the intervals seen in the complexes. This can indicate if there are any problems with the conducting system and also localise these.
The ECG trace
The nature of the change in membrane potential , alongside the direction in which these electrical changes occur , determines the morphology of the ECG trace.
Depolarisation towards an electrode gives a positive complex (upwards) on the ECG trace, whilst depolarisation away gives a negative complex (downwards). When measuring repolarisation , the opposite is generated; repolarisation towards a node is negative, and repolarisation away is positive.
The magnitude of the complex generated depends on the direction of the electrical current and the volume of tissue involved. The more direct and higher the electrical activity, the taller the wave will be.
There are characteristic wave patterns found within the ECG complex for a single cardiac cycle :
Fig 3 – A typical ECG trace as viewed from lead II
Components of the ECG trace
Using figure 3 above, we will now describe the key components of the ECG trace as viewed from lead II.
This represents atrial depolarisation. As the atria are relatively small and depolarisation is moving towards the lead, this is small upwards inflection.
This represents initial ventricular depolarisation, as the impulse spreads from the bundle of His . It is a small downwards inflection as it represents depolarisation, but the net impulse is indirectly away from the electrode.
This represents the bulk of ventricular depolarisation. The vector is directly towards lead II and represents a large mass, so gives a large, upwards inflection on the ECG.
As depolarisation spreads from the ventricular apex and turns superiorly, the S wave is generated. This is indirectly away from lead II, so despite the large mass it generates a small, downward inflection.
The T wave represents ventricular repolarisation. Repolarisation occurs away from lead II, but since the timing is dispersed as the ventricular tissue repolarises gradually, it creates a small, curved inflection.
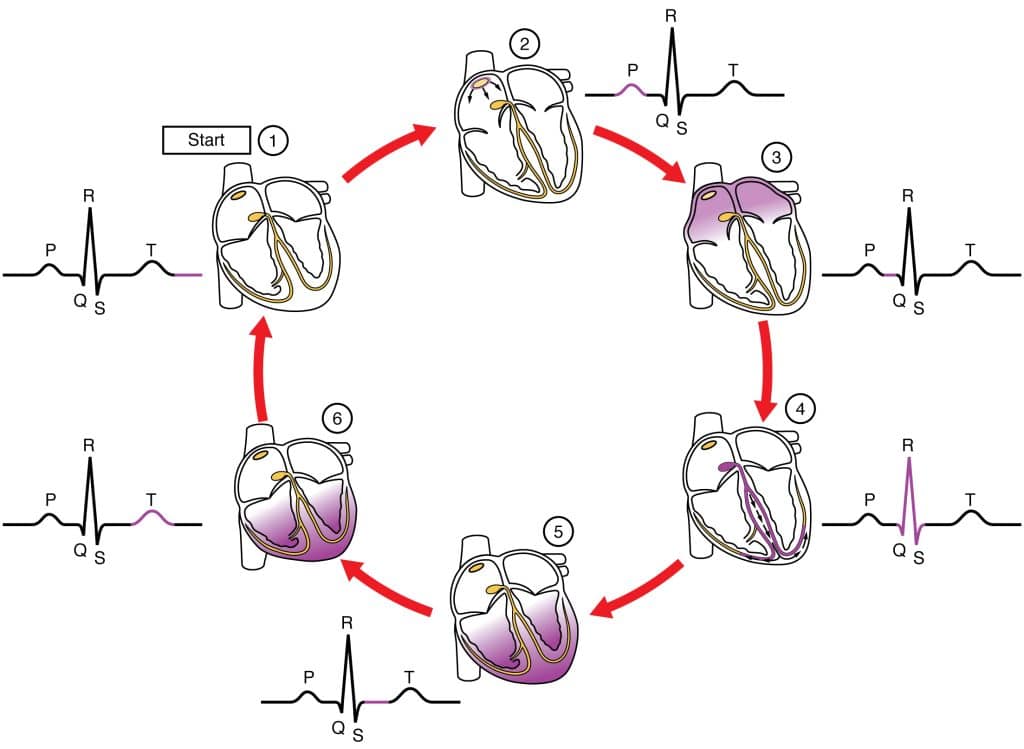
Fig 4 – The ECG tracing as viewed from lead II
The shape of the pattern seen on the ECG complex will vary dependent on the lead it is being viewed from. This is due the way in which the position of the lead will affect the direction from which it receives the impulse, and therefore the direction of the complex generated. Lead II is commonly used as the reference point for the ‘typical’ ECG trace.
Clinical Relevance – STEMI vs NSTEMI
The ECG is particularly useful in diagnosis of an ST elevation myocardial infarction (STEMI). A STEMI is defined as a complete occlusion of blood flow to a portion of the myocardium, resulting in ischaemia and full thickness infarction.
As the tissue dies it becomes leaky to electrolytes, leading to a partial depolarisation during the ventricular repolarisation period (ST segment). This leads to elevation of the ST segment, i.e. a STEMI.
In contrast, an NSTEMI is where there is partial occlusion of blood flow to the myocardium. This can lead to ST depression and T wave inversion, but not ST elevation. The mechanism behind this is complex and beyond the scope of this article.
The ECG is very useful in localising the region of infarction in a STEMI. There are characteristic leads which correspond to anatomical territories of the myocardium. If there is ST elevation in these particular leads it will indicate that there is infarction occurring in these regions. Using these leads the vessel most likely occluded can be identified, which is extremely useful in guiding treatment for the STEMI. This gives a useful non-invasive tool to localise pathology.
ECGs are most commonly measured using either 3 leads or 12 leads . The term 'lead' is slightly confusing, in that 12 lead ECGs actually only have 10 physical electrodes . These electrodes, however, generate 12 different 'views' of the heart. These 'views' are called 'leads'.
The shape of the pattern seen on the ECG complex will vary dependent on the lead it is being viewed from. This is due the way in which the position of the lead will affect the direction from which it receives the impulse, and therefore the direction of the complex generated. Lead II is commonly used as the reference point for the 'typical' ECG trace.
[start-clinical]
[end-clinical]
Found an error? Is our article missing some key information? Make the changes yourself here!
Once you've finished editing, click 'Submit for Review', and your changes will be reviewed by our team before publishing on the site.
We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy .
Privacy Overview
IMAGES
VIDEO
COMMENTS
The electrical stimulus travels down through the conduction pathways and causes the heart's ventricles to contract and pump out blood. The 2 upper chambers of the heart (atria) are stimulated first and contract for a short period of time before the 2 lower chambers of the heart (ventricles). The electrical impulse travels from the sinus node to ...
Print. The electrical system of the heart is critical to how it functions. It controls the electrical impulses that cause your heart to beat and their conduction, which organizes the beating of your heart. The movement of electrical signals across the heart is what is traced on an electrocardiogram (EKG).
Step 1: Pacemaker Impulse Generation. The first step of cardiac conduction is impulse generation. The sinoatrial (SA) node (also referred to as the pacemaker of the heart) contracts, generating nerve impulses that travel throughout the heart wall. This causes both atria to contract. The SA node is located in the upper wall of the right atrium.
The electrical signals that travel through your heart conduction system cause your heart to expand and contract. These contractions control how blood flows through your heart. ... It sends the electrical impulses that start the heartbeat. The SA node is in the upper part of your heart's right atrium. It is at the edge of your atrium near your ...
Structure Graphical representation of the electrical conduction system of the heart that maintains the heart rate in the cardiac cycle. Electrical signals arising in the SA node (located in the right atrium) stimulate the atria to contract.Then the signals travel to the atrioventricular node (AV node), which is located in the interatrial septum.After a short delay that gives the ventricles ...
The parts of the heart conduction system can be divided into those that generate action potentials (nodal tissue) and those that conduct them (conducting fibers). Although all parts have the ability to generate action potentials and thus heart contractions, the sinuatrial (SA) node is the primary impulse initiator and regulator in a healthy heart.
The original electrical impulse travels from the sinus node across the cells of your heart's right and left atria. The signal travels to the AV node (atrioventricular node). This node is located between the atria and the ventricles. In the AV node, the impulses are slowed down for a very short period.
Components of the Cardiac Conduction System Sinoatrial Node. The sinoatrial (SA) node is a collection of specialised cells (pacemaker cells), and is located in the upper wall of the right atrium, at the junction where the superior vena cava enters. These pacemaker cells can spontaneously generate electrical impulses.The wave of excitation created by the SA node spreads via gap junctions across ...
The electrical impulse begins at the SA node, located in the right atrium. The electrical activity spreads through the walls of the atria and causes them to contract. The atria and ventricles work together, alternately contracting and relaxing to pump blood through the heart. The electrical system of the heart is the power source that makes ...
The electrical signal spreads through the chambers of the heart. First, the atria are activated. The electrical signal then travels down through the conduction pathways to the heart's ventricles. This causes them to contract and pump out blood. The electrical signal then travels from the sinus node to the atrioventricular node (AV node).
Your body uses electrical impulses to control when your muscles flex and relax, and your heart is no different. However, your heart needs to do this 24/7, whether you're asleep or awake. To do this, it relies on a specific part of your nervous system called the autonomic nervous system. This is the unconscious part of your nervous system, and ...
The impulse takes approximately 50 ms (milliseconds) to travel between these two nodes. As the impulse reaches the atrioventricular septum, the connective tissue of the cardiac skeleton prevents the impulse from spreading into the myocardial cells in the ventricles except at the atrioventricular node.
The heart's electrical system. In the simplest of terms, the heart is a pump made up of muscle tissue. The heart's pumping action is controlled by an electrical conduction system that coordinates the contraction of the heart chambers. ... The original electrical impulse travels from the sinus node across the cells of your heart's right and left ...
When the electrical impulse reaches the atrioventricular node (3), it is delayed slightly. The impulse then travels down the bundle of His (4), which divides into the right bundle branch for the right ventricle (5) and the left bundle branch for the left ventricle (5). The impulse then spreads through the ventricles, making them contract.
The electrical signal spreads through the chambers of the heart. First, the atria are activated. The electrical signal then travels down through the conduction pathways to the heart's ventricles. This causes them to contract and pump out blood. The electrical signal then travels from the sinus node to the atrioventricular node (AV node).
Conduction is how electrical impulses travel through your heart, which causes it to beat. Some conduction disorders can cause arrhythmias, or irregular heartbeats. Three common conduction disorders are: Bundle branch block. Normally, electrical impulses travel down the right and left bundle branches of the ventricles at the same speed.
Figure 17.3.3 17.3. 3 illustrates the initiation of the impulse in the SA node that then spreads the impulse throughout the atria to the atrioventricular node. Figure 17.3.4 17.3. 4: Cardiac Conduction. (1) The sinoatrial (SA) node and the remainder of the conducting system are at rest.
The bundle of His is a collection of heart muscles cells specialised for electrical conduction. These cells receive input from the AVN. 1,4,5; The bundle of His branches into the left and right bundle branches which travel down the interventricular septum. Branches of the bundle of His propagate impulses to the left and right ventricles ...
In order for the heart to squeeze and pump blood, it needs a sort of spark plug, an electrical impulse, to start a heartbeat. The electrical impulse starts on the right side of the upper chamber in an area called the sinus node. The sinus node is the normal pacemaker of the heart and controls the heart rate. The heart normally beats faster when ...
The impulse takes approximately 50 ms (milliseconds, thousandths of a second) to travel between these two nodes. The relative importance of this pathway has been debated since the impulse would reach the atrioventricular node simply following the cell-by-cell pathway through the contractile cells of the myocardium in the atria.
The electrocardiogram (ECG) is used to trace the electrical activity in cardiac tissue. It looks at how electrical impulses travel through the heart from various angles. It is used clinically to identify and locate pathology within the cardiac conducting system and within cardiac muscle.. This article covers the physiology underpinning ECGs, as well as explaining pathological ECG traces and ...
Conduction is how electrical impulses travel through your heart, which causes it to beat. Some conduction disorders can cause arrhythmias, or irregular heartbeats. Three common conduction disorders are: Bundle branch block. Normally, electrical impulses travel down the right and left bundle branches of the ventricles at the same speed.
Conduction is how electrical impulses travel through your heart, which causes it to beat. Some conduction disorders can cause arrhythmias, or irregular heartbeats. A bundle branch block is a common conduction disorder. Normally, electrical impulses travel down the right and left branches of the ventricles at the same speed.